This is the 3rd part of principles of entrainment – please see entrainment -1 and entrainment -2 before you read this if not already done.
Before going further, we need to understand the concept of fusion.
As per the literal meaning this is about some thing blending together. In EP, this is mostly applied to surface ECGs -but intra-cardiac electrograms also can have fusion.
So what is fusion in ECGs? It is basically the combined effect of two or more foci of depolarization on the ECG. Lets look at very obvious example – Pre-excited ECG of WPW. In this, when a sinus beat comes down, it will go thru the conduction system as well as the accessory pathway. The contribution by the AP will give rise to the delta wave and the rest of the QRS will be by the conduction system. In the end, we have a fused complex of the delta wave with the QRS complex. If we remove the accessory pathway conduction – we have a pure QRS complex – the message here is that to identify fusion, a difference in the ECG morphology must be seen – therefore for practical purposes, most attempts at identifying fusion is applied to QRS complexes -not P waves as identifying a fused (different) p wave can be challenging. Read it carefully : if you cannot see a difference in ECG morphology, then there is no manifest (apparent) fusion !
In entrainment this refers to the combined (fused) appearance of ECGs during pacing.
Let’s work it out by using the following diagram. This is a bit different from the previous cartoons that we have seen and is closer to the structure of an actual tachycardia circuit – i.e. a scar VT circuit. But the same principles apply – there is a re-entrant circuit and there is an excitable gap we would like to penetrate. The major difference is that we now we consider the origin of the surface ECG and also look for fusion.
Note :For surface ECG fusion, it is expected that a full 12 lead is used for analysis as at times there can be subtle differences which may be missed if lesser number of leads are used.
The tachycardia circuit consists of a slowly conducing narrow channel confined by two zones of scarring. This sets up a re-entrant circuit (see re-entry) . The ECG during tachycardia is generated by the orthordomic wavefront exiting at one end of the channel.
Re-entrant circuit. Narrow channel of slow conducting tissue separated by two scar zones. The end marked as "Exit" denotes where the tachycardia comes of out the channel to enter the rest of the myocardium and perpetuate. This exit site is also the "focus" where the surface ECG begins as this site is exposed compared to the hidden channel.
Now assume that we place a catheter at the very exit site and pace slightly faster than the tachycardia cycle length as shown :
Pacing at the site of exit. The paced orthodromic wave exits at the native tachycardia exit (as the catheter is there) and the antidromic wavefront collides with the active wave of the previous beat. The paced ECG will be same as the tachycardia ECG as the paced site same as the native tachycardia exit site - i.e. there will be NO manifest fusion of the ECG. (In other words the ECGs of native and paced tachycardia will be same - no difference )
The same thing would happen if we pace within the channel. Since the surrounding myocardium cannot be capture (i.e. scar), the surface ECG will be dependent on the exiting tachycardia at the exit. Again in technical jargon, nomanifest fusion of the surface ECG!
Pacing within the channel. Since the channel is "protected" by scar tissue, the surrounding myocardium is not captured and the paced orthodromic wave will exit at the usual exit. Therefore the paced ECG will look similar to the native tachycardia ECG
Lack of any change in the tachycardia morphology during pacing (i.e. No manifest fusion of the ECG) – but fulflling other criteria for entrainment is called concealed entrainment
Now lets see what will happen if we pace on the outer myocardium (as would be a common practical scenario when we are looking for the circuit – aka pacing at random places with a mapping catheter).
The pacing site is on a out part of the circuit. Once paced, the antidromic wave will collide with the previous beat active front. The orthodromic wave will travel forwards in the circuit. The surface ECG would be a fusion of the ECG from the paced myocardium and the tachycardia wavefront exiting at the exit. The observation that we make is a difference in the paced ECG compared to the native tachycardia ECG - so we say there is "manifest fusion"
A similar ECG fusion is expected when pacing near the entrance to the channel. As the paced wavefront can go backwards (with the antidromic wave causing collision) the paced impulse contributes to the ECG by depolarizing the adjacent myocardium. Additionally the orthodromic wave travels via the channel and exits in the usual exit. Therefore the net ECG result is a fusion of waves generated by both of these sites.
As explained in the above diagrams, ECG fusion (a difference observed) is expected when pacing from an outer site. Once the paced wave penetrates the excitable gap, there would be continuous resetting of the tachycardia (antidromic colliding with the previous active front and orthodromic continuing as the tachycardia beat).
The main observation here is that ECG fusion is dependent on the site of pacing – therefore the absence of fusion in the surface ECG does not exclude re-entry. (in the next section entrainment – 4 we will see some practical examples – a very common entrainment that we do – pacing entrainment from the ventricle for AVNRT and AVRT do not show fusion at the surface ECG !!!)
Now what will happen if we pace at different faster rates? Look at the following diagram –
In this scenario, the pace site is out of the channel and therefore fusion is expected. The circuit tachycardia cycle length is 400 ms.
At rates only slightly faster (e.g. 390 ms), the paced wave takes a certain time to reach the ECG compared to the previous beat exiting at the exit. As we pace at faster rates, the paced wavefront comes quicker to surface ECG compared to the wave generated at the tachycardia exit. Therefore the "degree of fusion" varies with the paced rate - at rates close to the tachycardia rate - the ECG appears similar to the native tachycardia - and at much faster rates, is similar to the paced complex. How do we know what the pure paced complex looks like ? By pacing and noting the ECG when there is NO tachycardia !!! This variation of fusion during different rates of pacing is called progressive fusion and is a criterion to recognize re-entry.
Sometimes ECG demonstration of fusion may not be possible. For example, in atria, say during analysis of a atrial tachycardia, demonstration of fusion in P waves is very difficult.
However if we have additional electrodes in the circuit (or in the vicinity) we can demonstrate fusion at an electrogram level. This is shown in the following diagram. Basically with faster pacing, the collision site is pushed downstream and a strategically placed electrode will show this movement with changes in morphology (direction) and distance to paced spike
Identification of fusion in the electrograms. Again, the previous circuit with a TCL of 400 ms and we are pacing progressively faster. R1 electrode is recording at separate site. As shown in the diagram, faster pacing would result in the collision point being pushed away. In the first panel (A), the R1 electrogram belongs to the previous beat generated by the pace. In panel (B) the collision point of the antidromic wave and previous beat occur just at the electrode - and therefore there is a change in morphology and timing (arrowhead). In panel (C) the electrode is now recording the antidromic wave of the current pace - hence the short stim-to spike time. This timing difference (A to C) and change in morphology is considered electrogram equivalent of fusion
As demonstrated in the above diagrams, progressive fusion is an important criterion to prove re-entry. Unfortunately not all pacing attempts demonstrate ECG fusion as fusion is dependent on the site of pacing.However one can try to look for evidence of electrogram level fusion to identify re-entry.
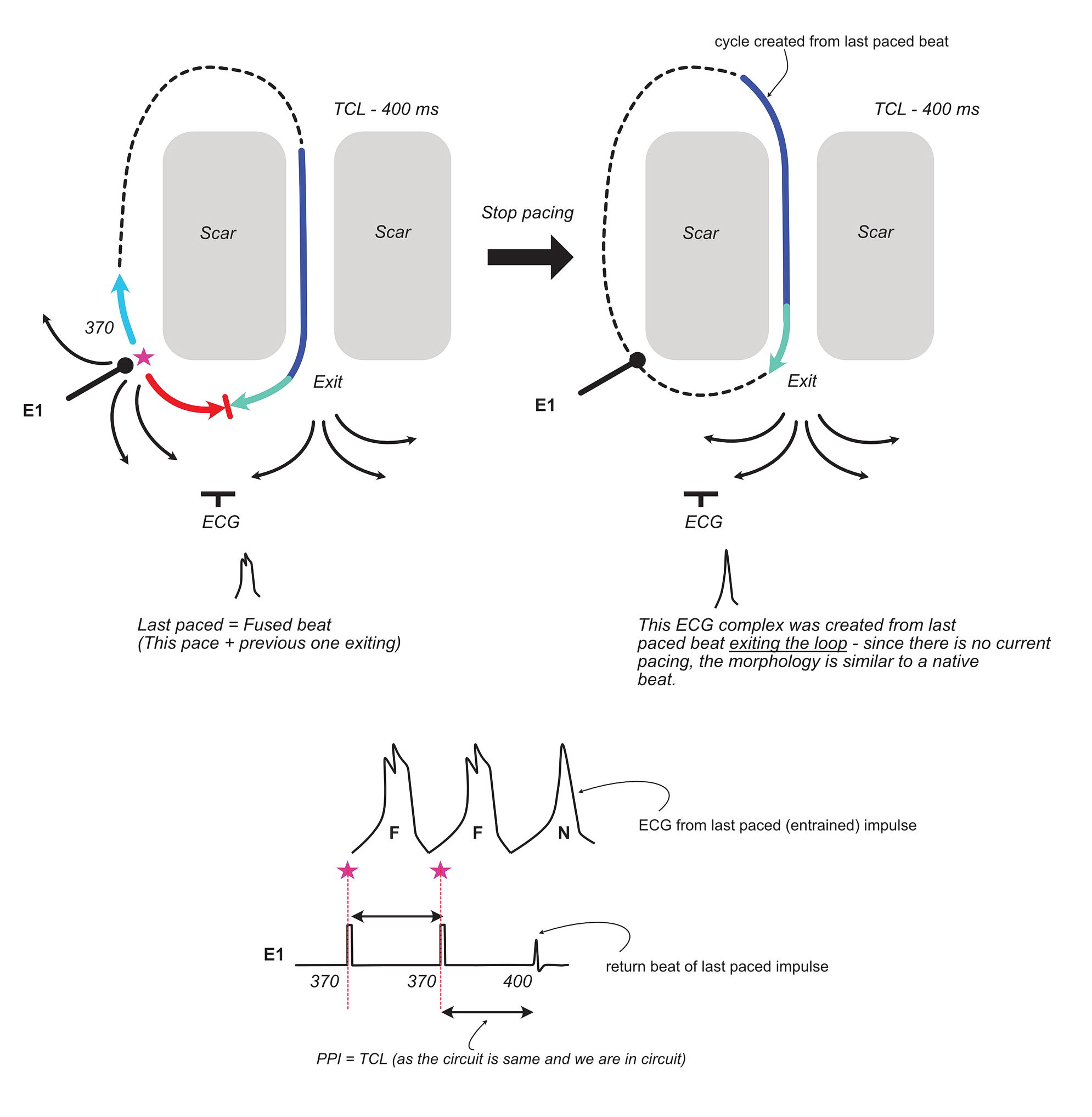
To conclude the discussion on ECG fusion, lets look at what happens when we abruptly stop pacing –
Previous circuit with a native TCL of 400 ms being paced at 370 ms within the circuit and sudden cessation of pacing. The last paced beat is fused at the pacing impulse also contributes to the ECG - but when the cycle that was initiated by that pace exits the loop, it will be similar to the native tachycardia beat as we have not stopped pacing. (i.e. nothing to fuse with). Looking at the pacing electrode recording we see that the last returning beat forms the Post pacing interval and is in the native tachycardia cycle length.
In addition to the fact that the ECG of the last cycle initiated by the paced beat appears like the native beat (no fusion), the other important takeaway is that the last beat cycle length is equal to the tachycardia cycle length (if we are in the circuit). In the original description of this phenomenon, it was stated that the last beat (also called the entrained beat) is at the paced cycle length – but it is obvious from the above that it has to be at the native cycle length and this has been proven in studies on human VTs
Now to the last bit – before we consolidate what we have learnt so far.
What will happen if we pace very fast than the tachycardia cycle length – i.e. make our paced beat enter the excitable gap very early?
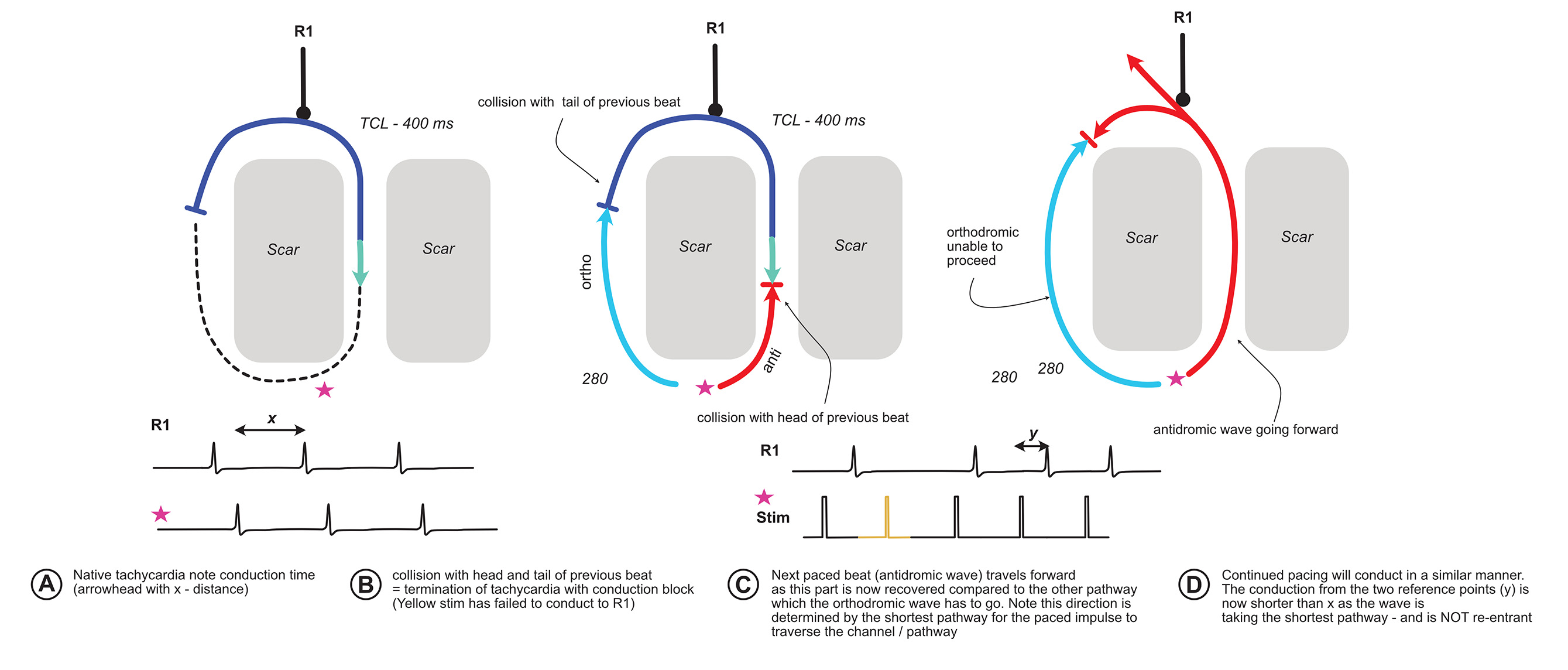
Lets work this out with the following diagram :
Conduction block with interruption of tachycardia. Again our same circuit with a TCL of 400 ms. A paced train at 280 ms will enter the the excitable gap very prematurely. This will travel antidromically and hit the head of incoming previous wave and also collide orthodromically with the refractory tail of the previous wave. The effect would be termination of the tachycardia and a non conducted stimulus to R1 (yellow). If we continue to pace at this speed, the next beat will travel antidormically (as the orthodromic side is yet to recover). This will continue until we stop pacing. The conduction of the paced beat is now NOT re-entry. Note the x and y distance is the conduction time from the two reference points (stim electrode and R1). x is longer as it goes in the same direction of the tachycardia. y is shorter as now it is simply taking the shortest route through the channel and orthodromic wave of the paced beats are getting blocked by colliding with the antidromic wave. So there is NO reentry now.
The critical observation of the above is that when there is termination of tachycardia with a conduction block, the subsequent paced beats activate the circuit in a different direction. For this phenomenon to occur, initial tachycardia has to be re-entry.
A relevant real life example is pacing the ventricle in orthodromic AVRT. Once a critical pacing speed is achieved, the tachycardia terminates with a block to the atrium and ventricle. The subsequent paced beat enters the atrium via the AV node limb (because our site of pacing is near the RV apex). If we have sufficient catheters, we will be able to see the different activation sequence (VAH before block vs VHA after block) AND the timing difference shorter.
Oh by the way, ICDs terminate re-entrant VT with anti-tachycardia pacing (ATP) using this mechanism.
The key takeaway is termination of tachycardia with conduction block. For large circuits where we can strategically place catheters, we may observe different activation sequence and shortening of conduction times.
Now lets recap what we learnt above in the form of official criteria for entrainment. Waldo originally described 3 criteria and the fourth one was added later by Henthorn. I deliberately avoided stating these criteria at the beginning to facilitate understanding the principles behind these criteria.
Pacing during tachycardia yields constant fusion on the surface ECGexcept for the last captured beat, which is not fused
Progressive fusion while pacing at different rates
Pacing termination of tachycardia yields localized conduction block followed by activation of that site with a shorter conduction time
Change in conduction time and electrogram morphology when pacing at 2 different rates (progressive fusion at electrogram level)
Now that you know the mechanisms, the criteria are self explantatory. Proving one or more criteria in a given tachycardia confirms its mechanism as re-entry.
With regard to the first criterion, identification of proper fusion is essential – sometimes this is not straightforward. If there is no change in surface ECG morophlogy – but yet the tachycardia fullfills other criteria, then we have concealed entrainment (i.e. entrainment without apparent ECG fusion). Concealed entrainment should be strictly applied to surface ECG as even in the absence of ECG fusion, 4th criterion may be fulfilled.
The conduction time clause (short) in the 3rd criterion is based on the fact that the paced beat travels via the antidromic route of the original circuit. However in real life other structures involved may add decremental properties to slow down and actually prolong the interval (the classic example being AV node dependent circuits) – the aim is to identify the different route compared to the native tachycardia
In the next section we will look at some practical examples of the above mechanisms at work