As the name implies, re-entry is something entering something in a repeated fashion. In arrhythmia, it is when a tachycardia is seen traveling (propagating) along an anatomical pathway.
Understanding what re-entry is and how re-entry tachycardia is formed is fundamental to understanding entrainment.Therefore this section will concentrate in what re-entry is and how re-entry is initiated.
Re-entry is one mechanism of arrhythmia and is the most fun type of mechanism. Other types include – triggered activity and automaticity (boring!) – why is reentry fun ? Because we can do things to it and most are potentially curable!
If you recall basic cellular electrophysiology, cardiac cells propagate impulses by depolarization not by direct conduction as in a electric circuit.
Depolarization and repolarization takes time (milliseconds). Therefore a spread of depolarization is followed by a tail of cells repolarizing. These repolarizing cells cannot excite until fully repolarized therefore they create a tail of refractory cells. The fully recovered cells in behind the refractory tail and the still not-depolarized cells in front of the wavefront are excitable and termed the ‘excitable‘ gap. The direction of the tachycardia depends on where the initial depolarization began and the anatomical tissue pathway.
Depolarizing wave. In green are the cells actively depolarizing. In yellow are the cells re-polarizing. The excitable (available for depolarization) form the excitable gap in front and back of the tachycardia wavefront.
Cardiac cells spread the depolarization to adjacent cells by gap junctions and this determines the microscopic direction of impulse conduction – however for practical purposes, macrosopcically, the impulse can travel in any direction as there are gap junctions all over the place. In some places (e.g. the Crista Terminalis) fiber orientation tends to direct the wave front.
For re-entry to occur, the depolarizing wavefront needs to come back on its own. For this to occur – there must be an anatomic obstruction that creates “circuit of tissue”. In real life these obstructions are either scar tissue or natural obstructions like valve rings, cavo-tricuspid isthmus etc.
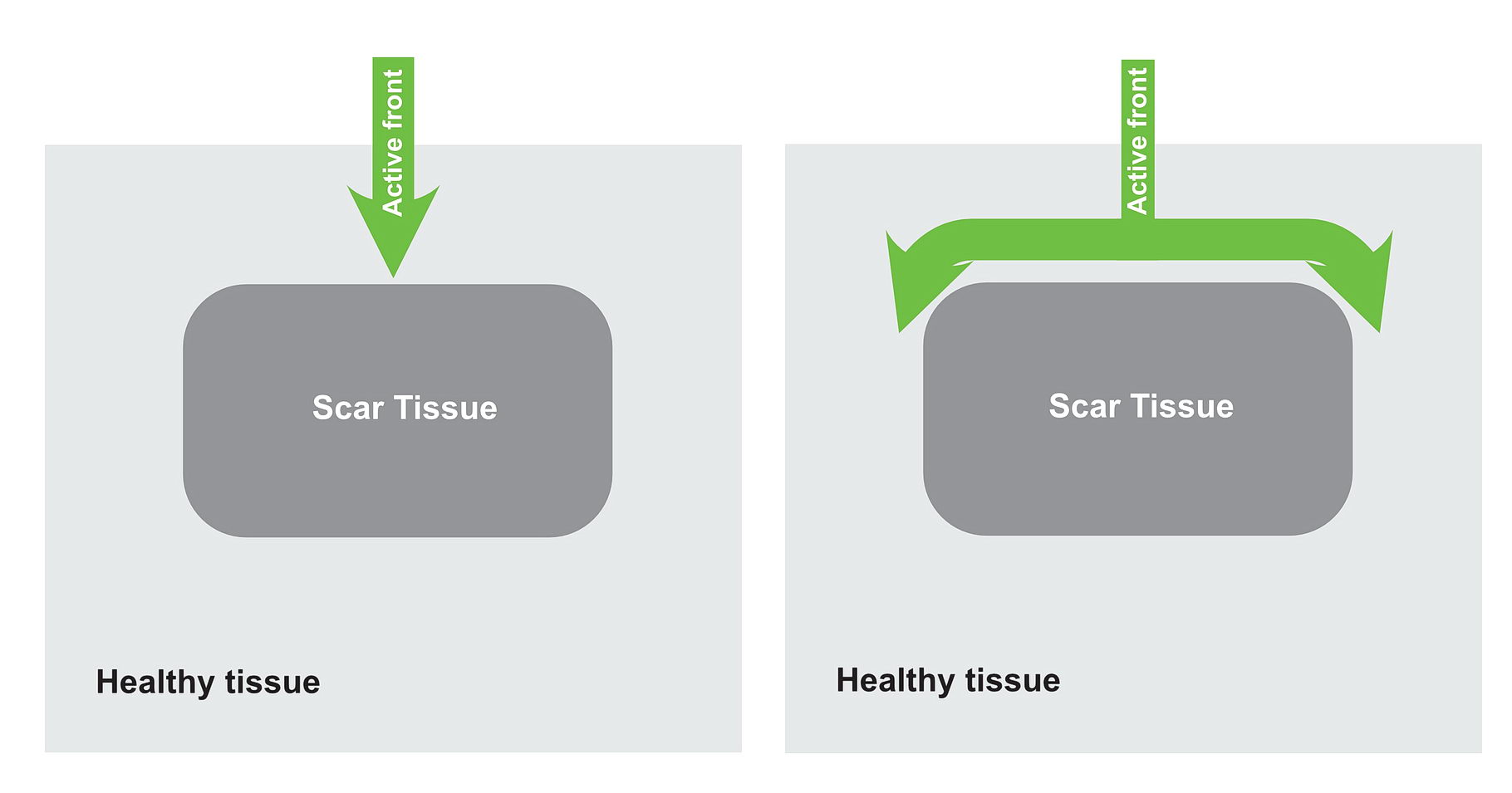
Lets look at the following diagram – which shows a anatomical scar within a blob of healthy tissue. What will happen if an impulse arrives at near the obstruction? Is re-entry possible?
Impulse arrives at the anatomical obstruction and travels on either side of it
Since the surrounding tissue is equally healthy, the impulse wave fronts travel in a similar manner around the obstruction and collide.
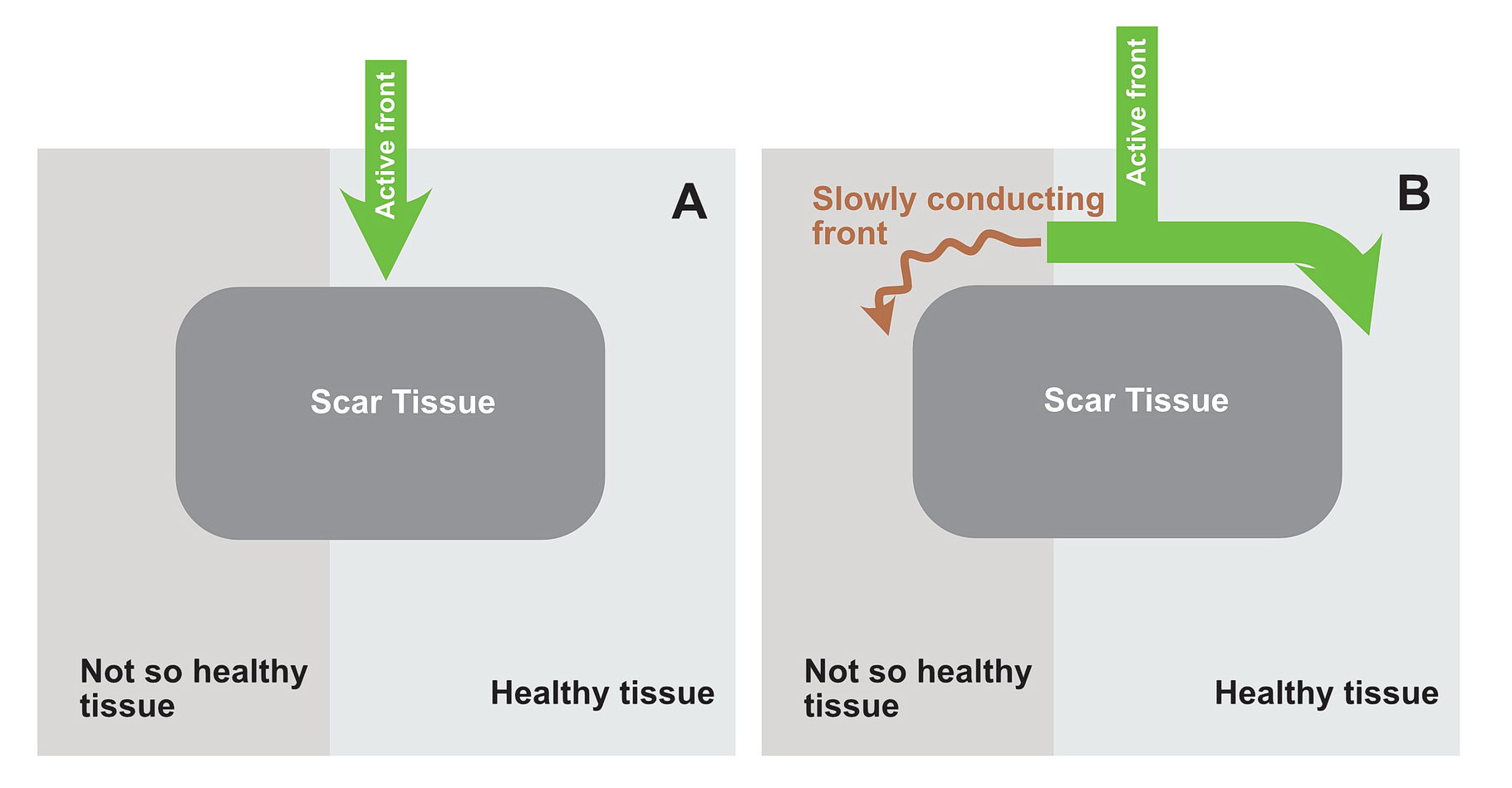
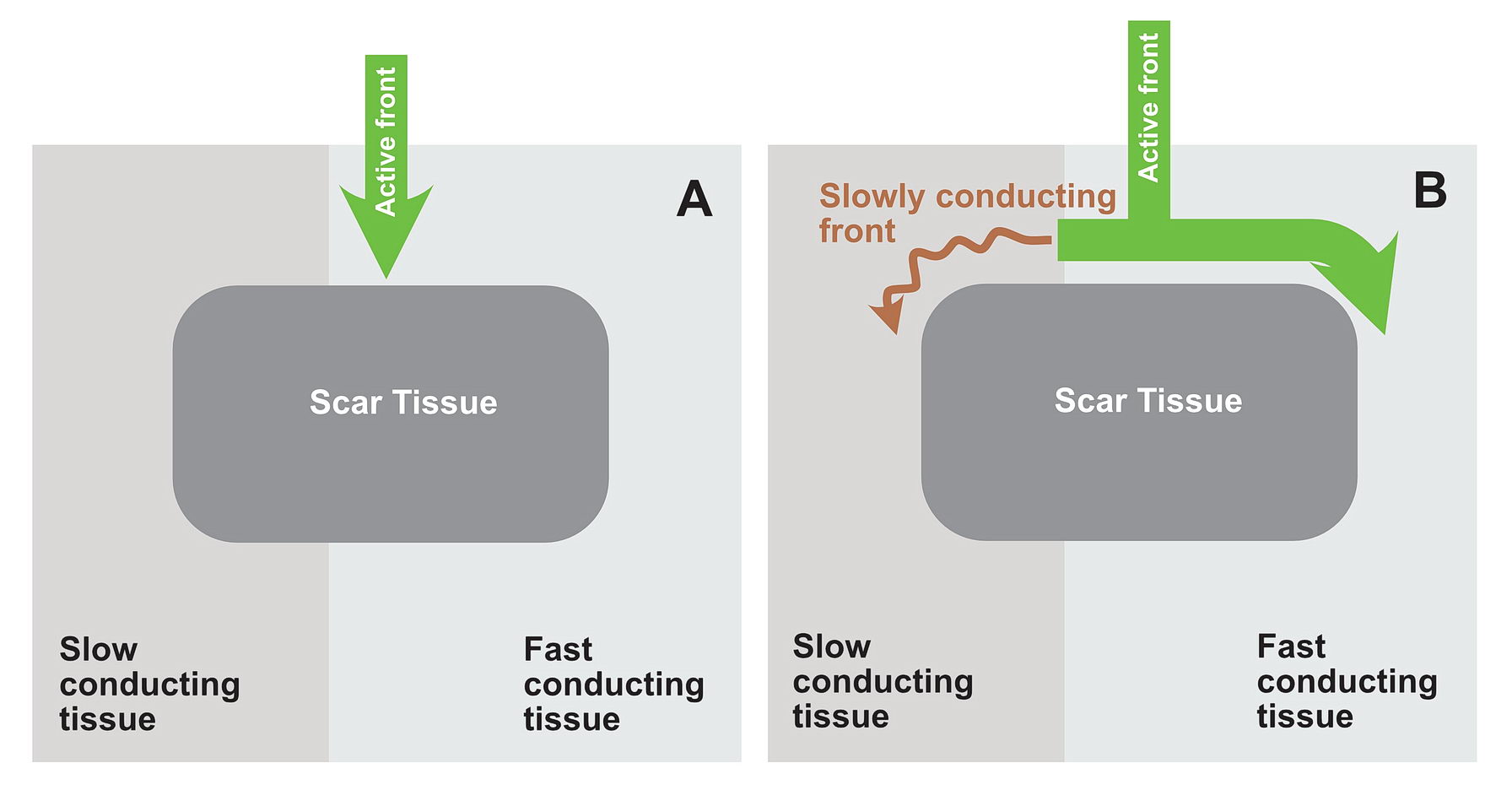
Now consider, the obstruction creating two pathways – which have different electrical properties. One can conduct fast and the other conducts slowly because of disease state.
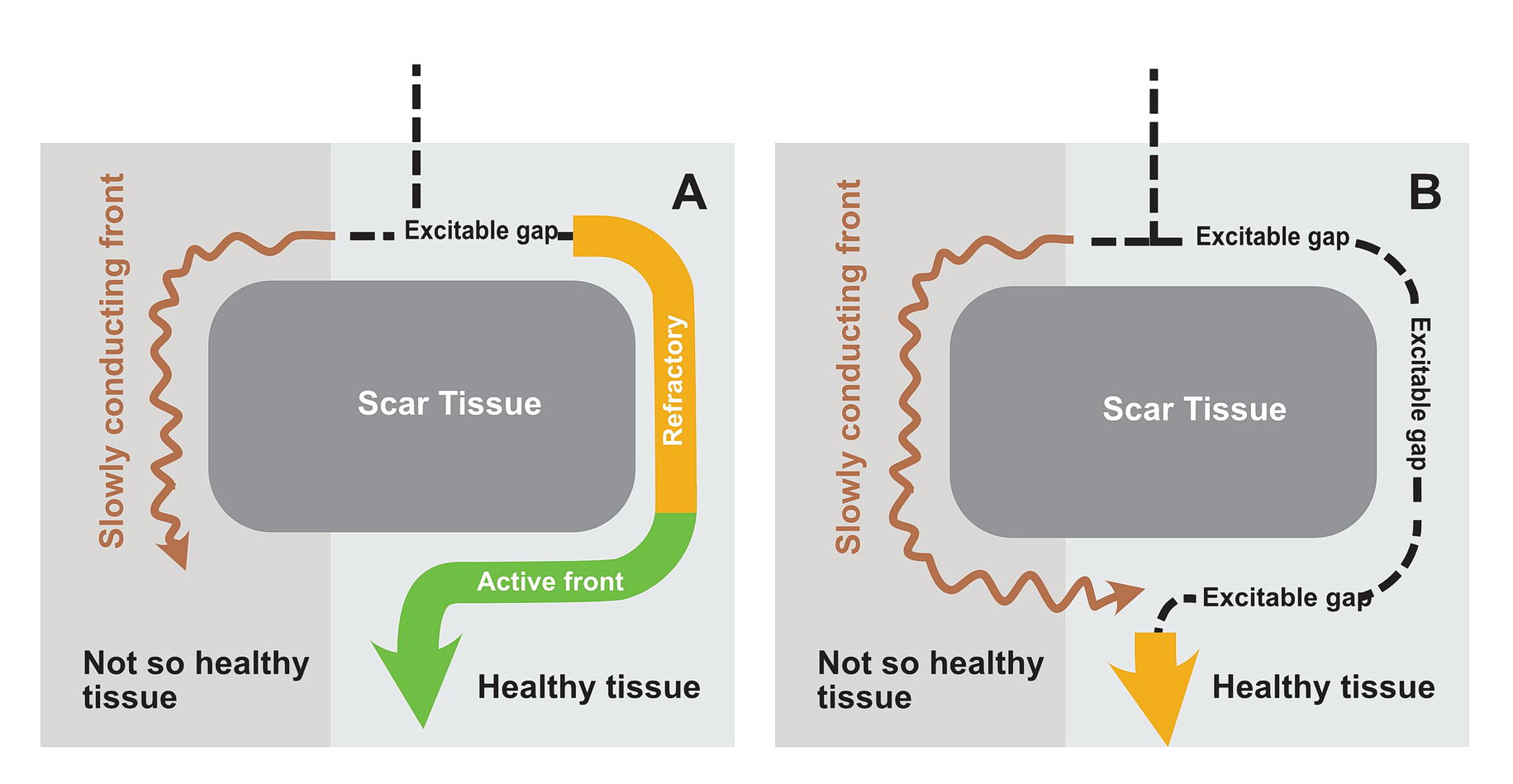
Note on the left side, the tissue is more diseased and therefore conduction is slow. Panel A and B show the incoming wavefront spreading on either side of the obstruction where the conduction via the disease side is slow
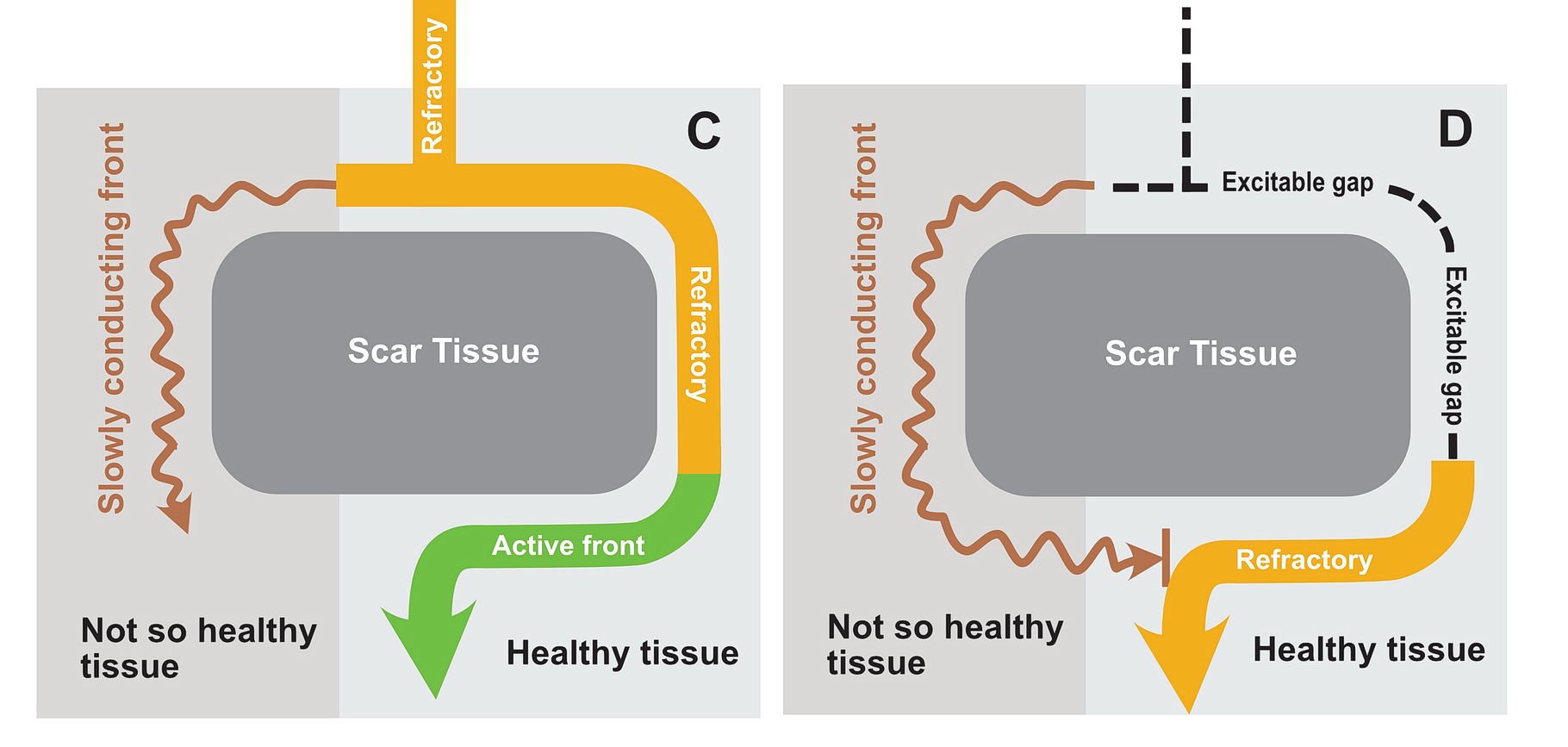
Panel C shows the wavefront on the right side (green) almost now gone beyond the obstruction. Meanwhile the conduction on the left side is progressing slowly. Panel D shows the wavefront now gone on the right side with the tissue remaining refractory - and most importantly the conduction which arrived via the slow pathway cannot enter the right side limb - because that limb is still refractory
In this situation as shown in the diagrams, there exists a potential for the wavefront coming via the slow pathway to re-enter the other pathway provided the tissue is not refractory.
If the conduction via the slow pathway is sufficiently slow, the other pathway might have enough time to recover and enable re-entry
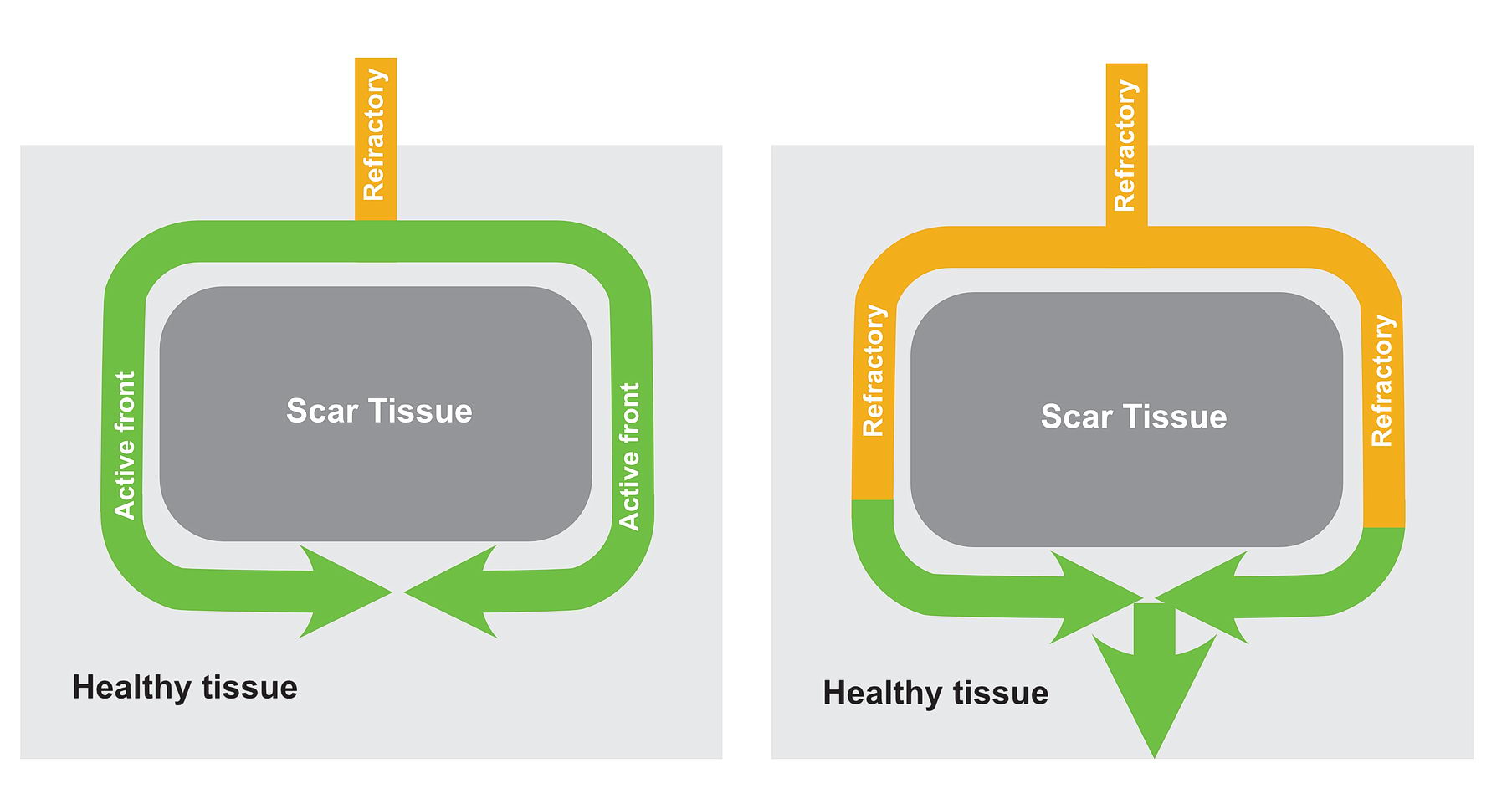
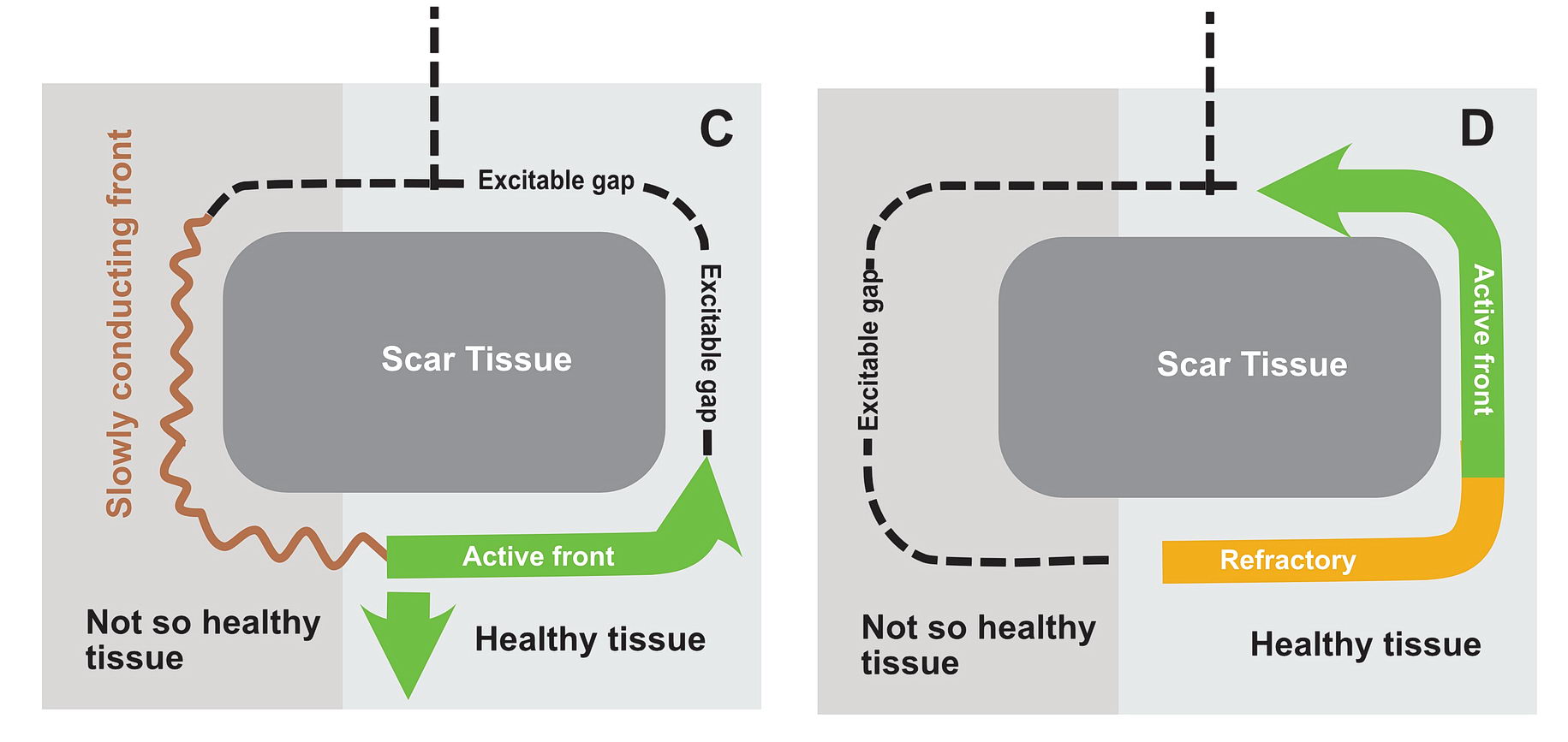
Panel A shows a wavefront approaching the obstacle and going on either side. The left side is diseased and conducting slowly. Panel B shows that on the right side, the wave front has gone off and the tissues have recovered and excitable.
Panel C shows, the wavefront which came slowly down the left side, now enters the right side because the tissue on the right has recovered. - thus setting up - re-entry as shown in panel D. As long as the refractory period is small on the right side and the wave is sufficiently delayed on the left side, this re-entry perpetuates.
In real life this would mean incessant tachycardia and fortunately it is rare. The common mode of initiation of tachycardia when this sort of substrate is present by creating a functional unidirectional block and presence of premature impulses.
Lets look at this in detail as this is a very important concept for arrhythmia initiation which we can also use in the EP lab.
The requirements are
Two sets of tissues – with different conduction properties
Separated by anatomy
Functional unidirectional block and premature impulse
Two sets of tissue with different conduction properties
This could be scar tissue (e.g. from a ischemic insult, surgery etc) or normal but “different” tissue separated by normal anatomical boundaries – the classic examples being the slow pathway (SP) in AV Nodal re-entry and Cavo Tricuspid Isthmus (CIT) In right atrial flutter.
The critical distinction between the two groups of myocardium should be different conduction properties. Usually this means one group conducts slows and recovers fast whereas the other group conducts fast and recovers slowly. In a normal heart, majority of the tissues are fast conducting and slow recovering. That’s why when there is myocardial injury, slowly conducting tissues form this type of arrhythmia zones- i.e. the scar forms the obstruction (anatomical separation) and the still alive tissue in the scar forms slowly conducting segments. Collectively this facilitates re-entry – especially with premature impluses as described below.
Slowly conducting tissue recovers fast and fast conducting tissue takes time to recover
Anatomical separation of the tissue groups
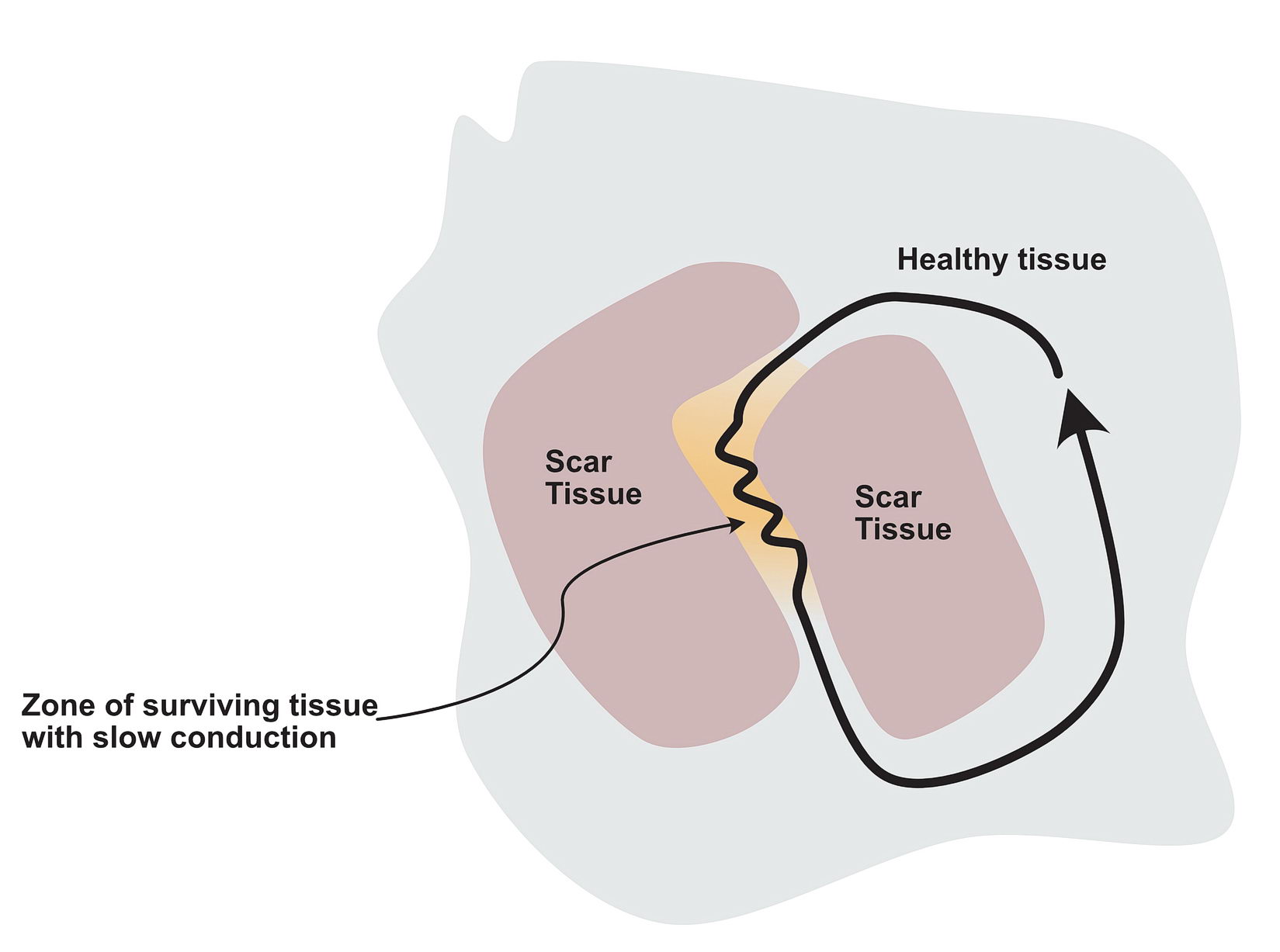
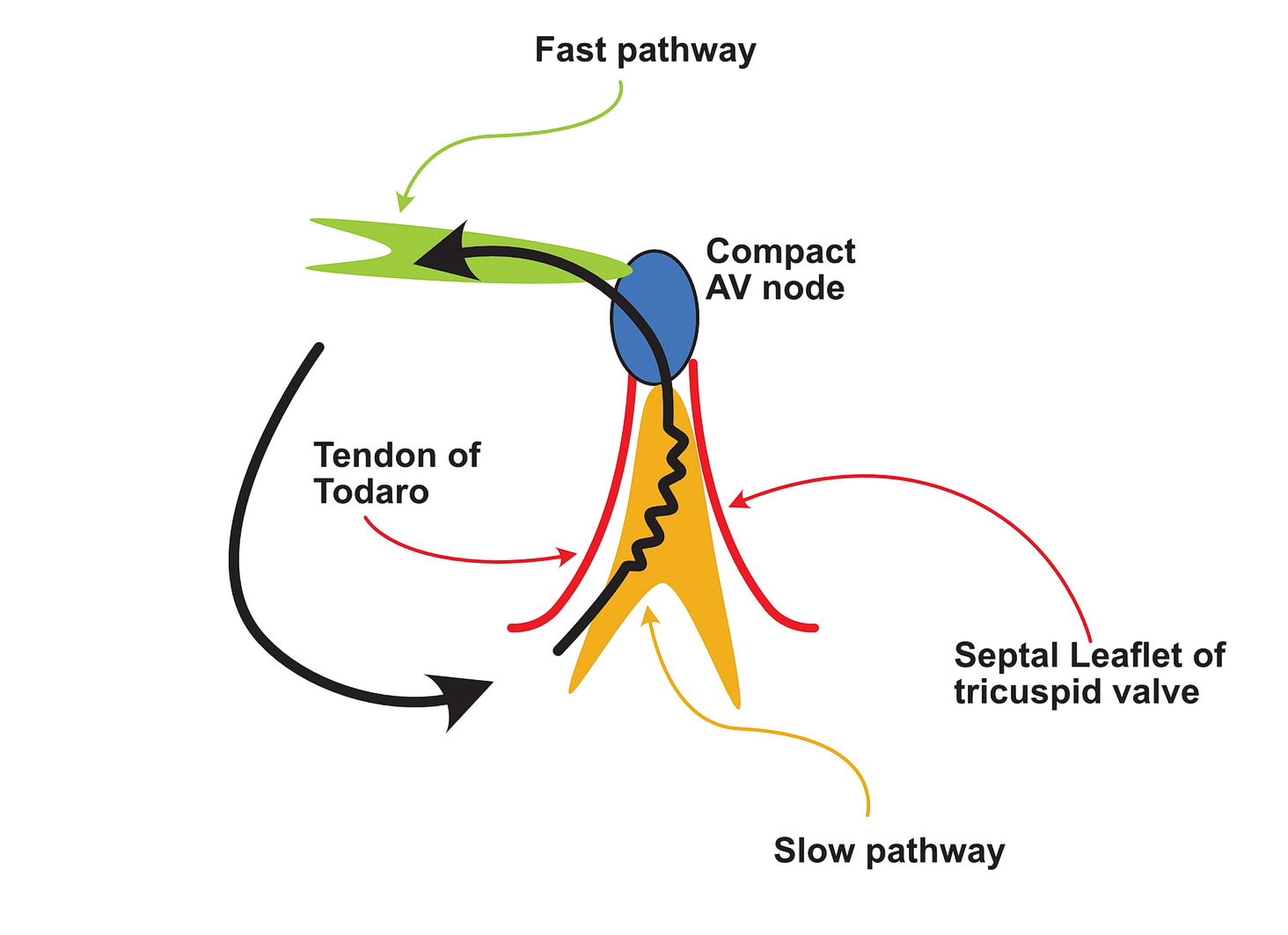
In a scar, a surviving but injured group of cells form the slow conducting tissue. Therefore the dead scar tissue forms the separation. However even in normal hearts, certain anatomical locations have differently conducting tissues which facilitate re-entry and they are separated by normal tissue with resistance to conduction. One good example is the slow pathway in AV nodal re-entry – where the slowly conducting tissue is bound by two barriers – the tendon of Todaro and the septal leaflet of the tricuspid valve (see figure). The other common place is the cavo-tricuspid-isthmus (CTI) where there is slow conduction and this facilitates re-entry. (see figure)
Re-entry circuit in scar tissue. The bulk of the scar is electrically silent but creates channels of surviving slowly conducting tissue. This facilitates re-entry
Re-entry circuit in AVNRT. The slowly conducting pathway (SP) shown in yellow is bound by the Tricuspid valve septal leaflet and the tendon of Todaro. This creates anatomic separation and slow conduction to facilitate re-entry
The cavo-tricuspid-isthmus (CTI) is a slowly conducting zone of tissues - bound anterior by the tricuspid valve ring and posterior by the Eustacian ridge of the IVC.
Functional Unidirectional Block and Premature Impulse
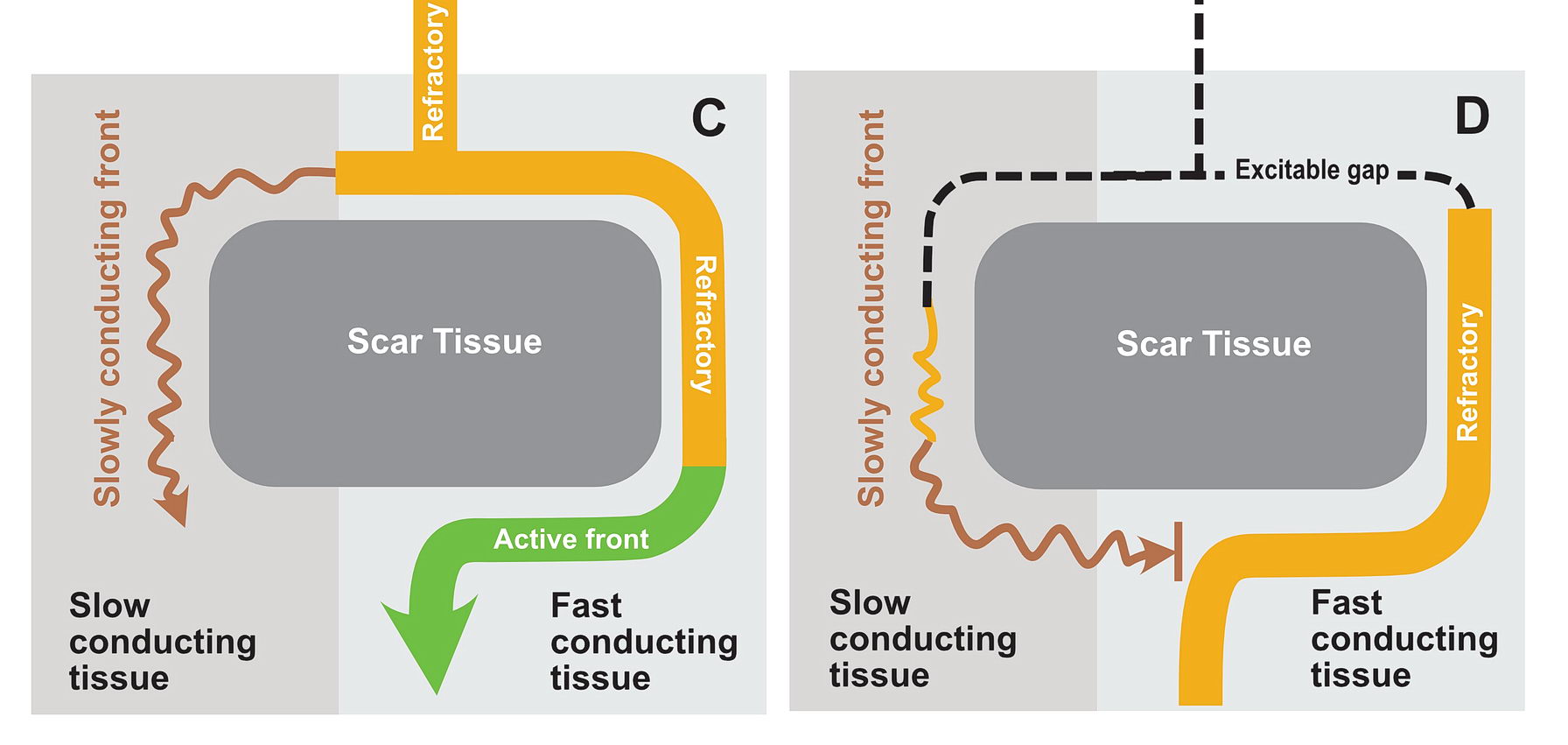
The premature impulse initiates the tachycardia loop by entering a functional unidirectional block. The following series of figures explain it.
A normal (green) impulse reaches the anatomic area and travels around it. The zone on the left side conducts slowly
Now the impulse reaches the distal part of the anatomic obstruction via the fast conducting (right) tissue and leaves the area (C). This conduction zone is now refractory. This refractory segment prevents the impulse slowly reaching via the slow zone from re-entering the fast zone - i.e. the fast conduction as created a functional block in that zone. (D)
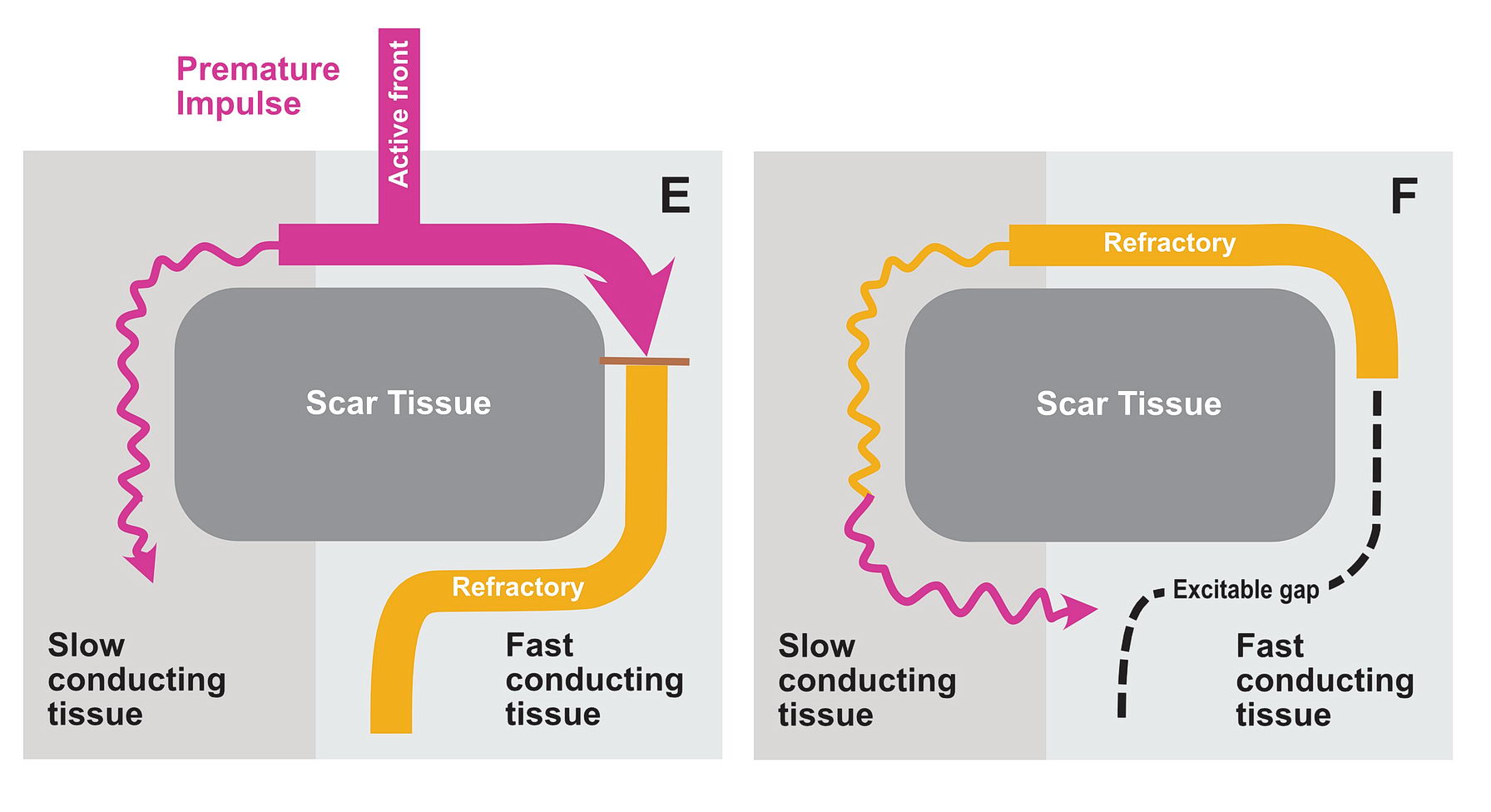
Now a premature impulse (purple) enters the area (E). It cannot go down the fast zone as it is still refractory and slowly comes down the slow zone as this has recovered. By the time it reaches the end of the obstruction zone, the fast zone has recovered and the wavefront enters the fast zone (E).
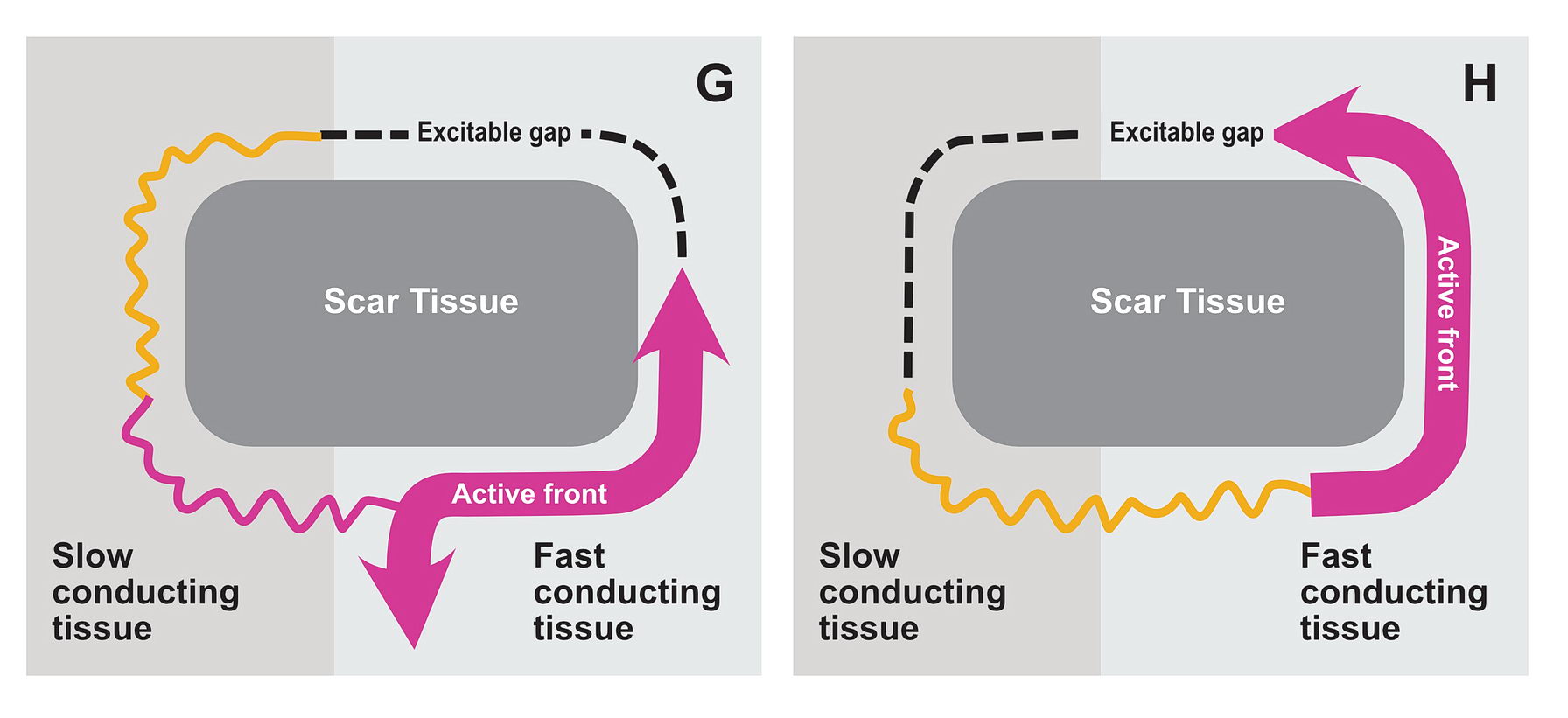
Now the wavefront can go back up the fast zone and re-enter the slow zone in a perpetual manner.
The functional unidirectional block is key for initiation of re-entry.
We routinely exploit this in the EP lab by putting premature complexes into the functional block to initiate tachycardia.
This also one mechanism how beta blockers reduce the incidence of arrhythmia – they prevent premature complexes which initiate re-entry
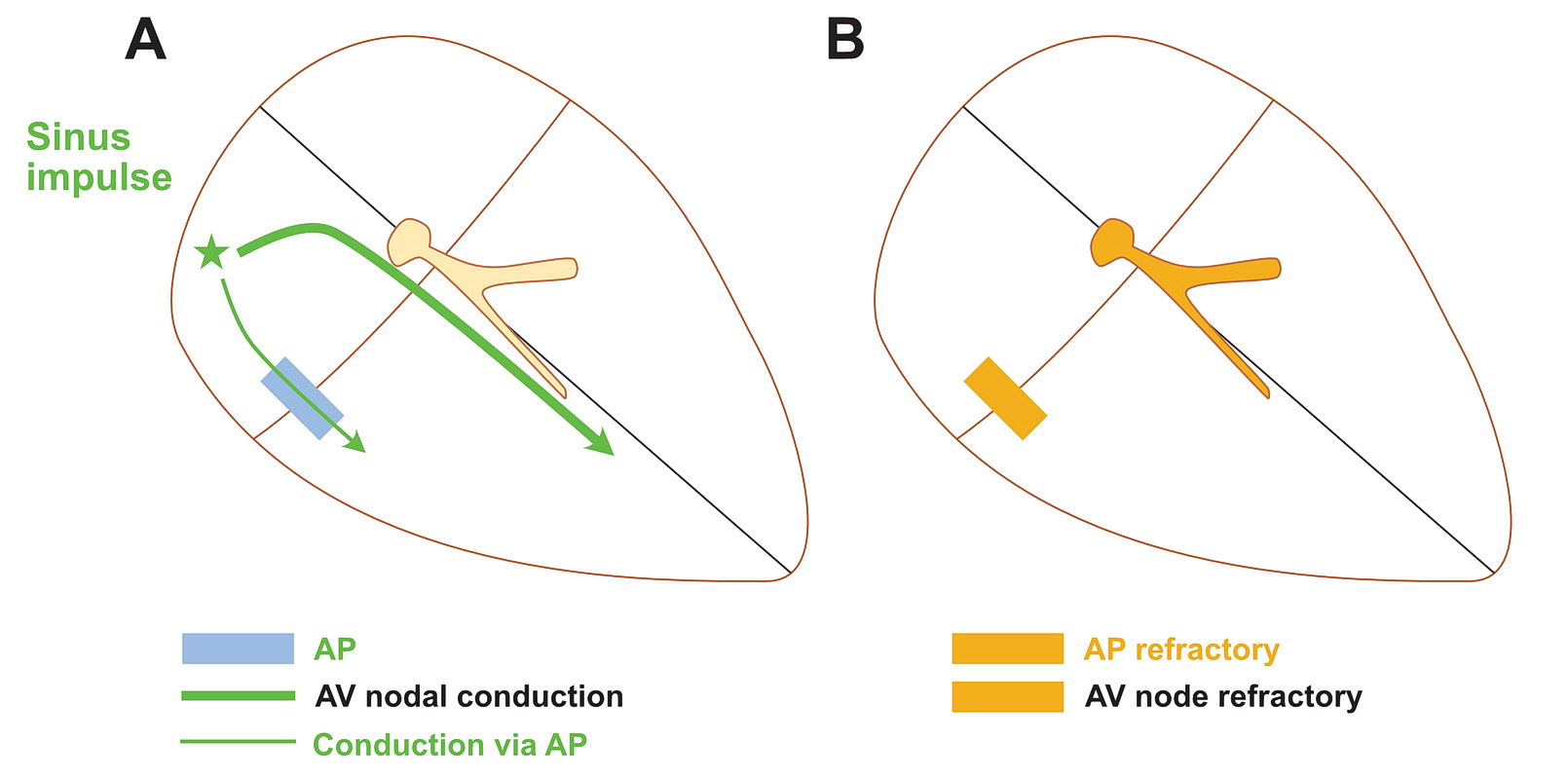
Although anatomically far apart, the same principlecan be applied for accessory pathway mediated tachycardia (i.e. Atrioventricular Re-entrant tachycardia AVRT). One limb is the AV node and the other limb is the pathway. Normal sinus rhythm maintains a functional block in either limbs depending on the relative speed of conduction in the two limbs. Therefore a correctly timed PVC or PAC can initiate re-entry by entering the excitable gap during this functional block. In the following example, we assume the common situation of fast conducting, slowly recovering accessory pathway.
A heart with an accessory AV pathway (AP). A sinus beat travels via the AV Node. In this case there is pre-excitation there is some conduction via the AP too. Some AP do not conduct antegradely and conduct retrograde only (concealed APs). Once the beat has conducted, the AP and AV node a refractory
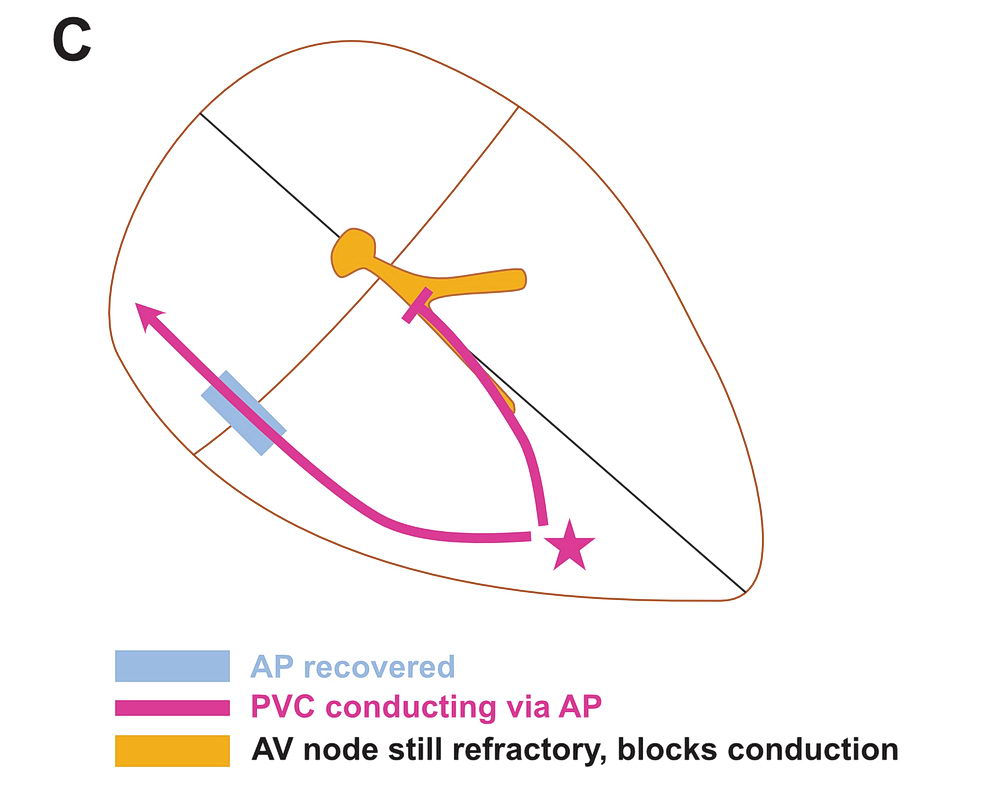
The AP recovers quickly compared to the AV Node. Now a premature ventricular complex (PVC) occurs and finds that the retrograde conduction via the AV Node is not possible and conducts via the AP back to atrium
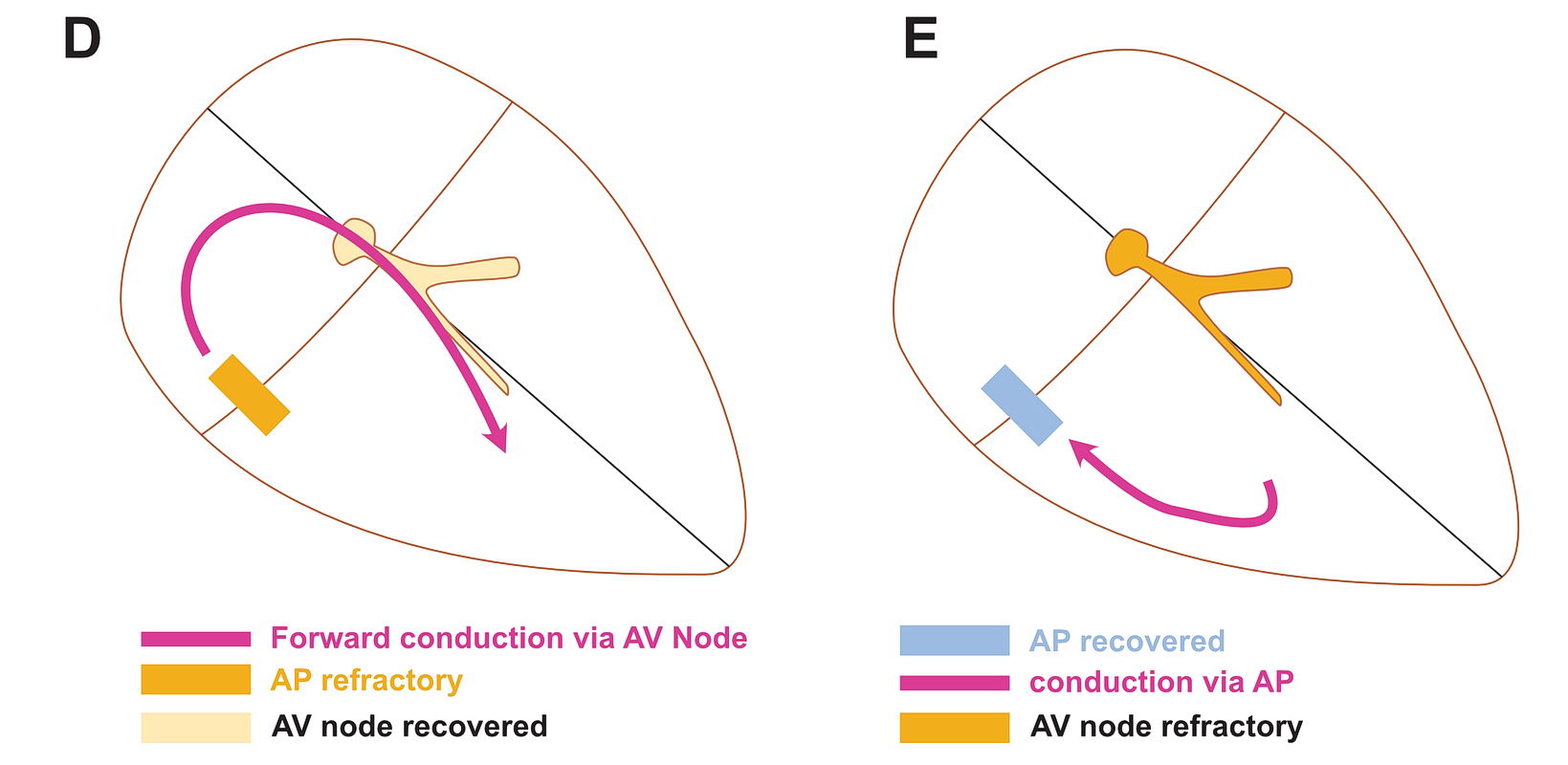
Now the AV node has recovered and the impulse comes back down the AV Node - setting up a perpetual circuit.
As shown above, PVCs can initiate tachycardia when the AV node is refractory. In addition, most APs conduct very happily from the ventricle to atrium – why? : Read the section on source-sink concept. Together taken (fast recovering limb and ease of conduction to V) is why extra-stimulus pacing in the ventricleeasily induces tachycardia in patients with WPW
The same can happen with PACs in the atrium – but it is unusual as favored direction of travel across the AP would be V to A. If it did travel the other way, it would initiate an antidromic AVRT.
If the AP conduction is slower than the AV node, then PACs can initiate orthodromic AVRT – but again finding such AP would be rare – like in the case of PJRT.
To recap, re-entry substrate requires two myocardial tissue segments of different conducting properties connected at ends but separated by an obstruction. The common way of initiating re-entry is by premature complexes entering the circuit when one segment is functionally blocked.
The difference in conducting properties would be one tissue with fast conduction & delayed recovery and the other one with slow conduction & rapid recovery
How this applies to various tachycardia types will be discussed in each type of tachycardia.