To identify the presence of an extra-anodal connection between the atria and the ventricle – i.e. an accessory pathway
Why?
As a maneuver in sinus rhythm when the presence of a concealed accessory pathway is suspected (e.g. for a short RP tachycardia)
Post ablation, to confirm complete abolition of retrograde conduction in an accessory pathway.
Principle
In normal a heart without any extra-nodal AV connection (i.e. no AV accessory pathways), the exclusive connection between the atrium and the ventricle is via the His bundle
The His bundle made up of conduction fibers enclosed in an insulating sheath. This sheath helps to maintain the structure of the His bundle and prevent current ingress or leakage.
However, if a sufficiently high current is applied to the His bundle, the insulation can be overcome, and the fibers directly stimulated which is called His bundle capture.
How do we do it – by pacing via the quadripolar (or whatever) catheter placed near the His bundle during the EP study. Now the impulse will travel via the conduction system to the ventricles and activate the ventricle – in a similar manner how a sinus beat gets into the ventricle. Therefore the resulting QRS complex should be narrow. However, as the catheter is also in contact with the adjacent myocardium, there will be some myocardial capture as well- therefore the resultant QRS complex is a fusion of myocardial conduction and impulse arriving via the conduction system – hence the actual QRS complex is not perfectly narrow – but will be fairly narrow.
Additionally, there will be retrograde conduction to the atrium – which can be detected if there is catheter recording the atrial signal
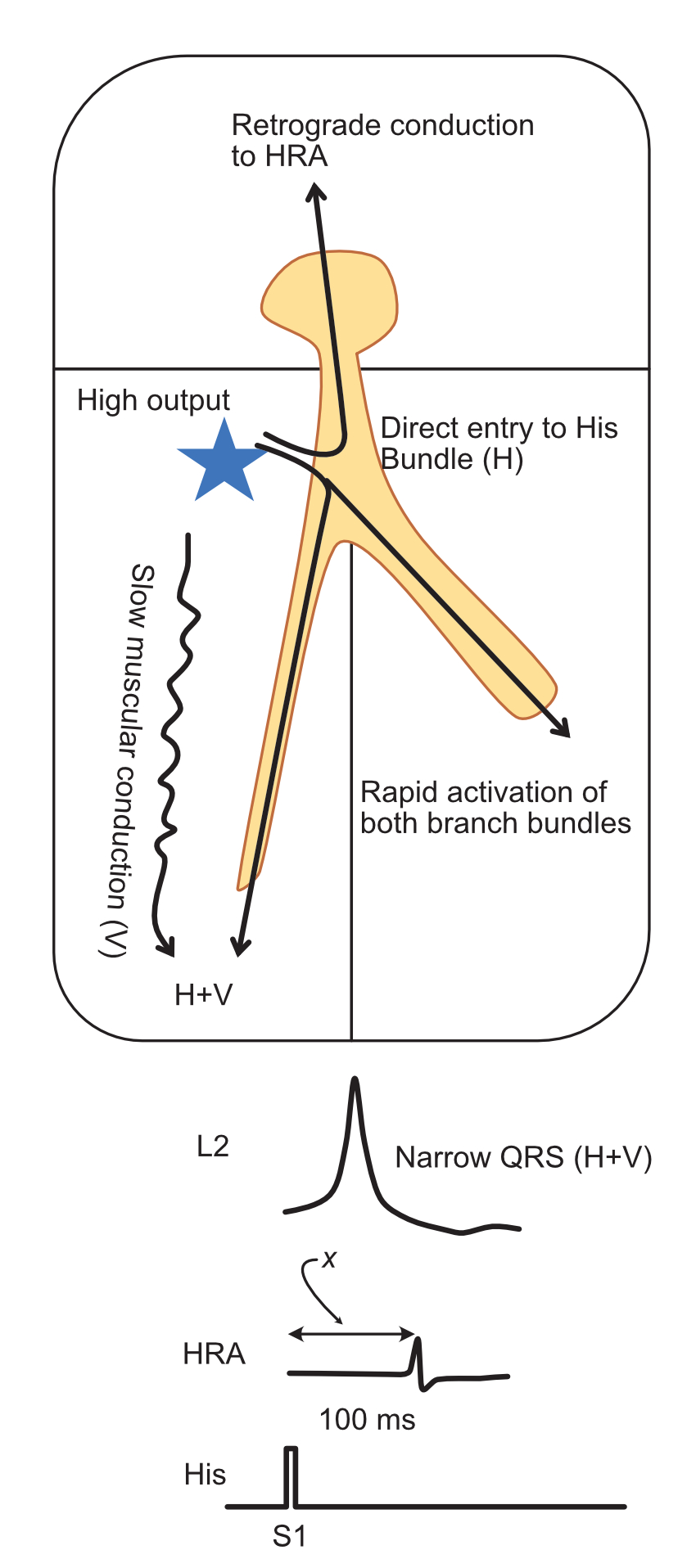
Stimulation at high output (typically 20 mA) near the his bundle. The QRS complex is a fusion of rapid purkinje conduction and slow myocardial conduction (H+V). The atrial catheter (HRA) records retrograde conduction and therefore we have the stimulus to – A time (x)
Parahisian pacing - loss of His bundle capture at low output – marked by sudden widening of the QRS complex. It is also marked by a prolongation of the stimulus – A time.
Critical observation : Observing the widening of QRS is the most critical step of this maneuver as this is the surrogate marker that we use to determine loss of capture of the His bundle. Since the pacing catheter is in the septal myocardium, sometimes careful observation of several ECG leads is necessary to verify change in QRS width
To recap, in a normal heart – loss of His bundle capture (as demonstrated by widening of QRS leads to an increase in stimulus to A time – this is termed as a Nodal Response to parahisian pacing.
Nodal response. The key observations are the (1) widening of QRS and (2) increase in stimulus to A time (x)
Now consider a patient with a accessory pathway. The His bundle response to pacing at high and low output will be the same. However since now there is “leak” to the atrium via the AP, the time for the stimulus to get to the atrium is now NOT dependent on retrograde conduction via the His. Therefore the stimulus to A time will be similar ! In other words, the lack of a difference in stimulus to A time when there is a change in QRS morphology indicates the presence of an accessory AV connection. This is termed an Extra-nodal response
Extra-nodal response. Regardless of what is happening to his bundle activation (i.e. what we see as a wide or narrow QRS), the stimulus to A time remains same as there is pathway conduction
Lack of difference in the stimulation to Atrium time during a change of morphology of the QRS complex (during reduction of output) – suggests a presence of a accessory pathway.
In Practice
Identify a good pair of electrodes to pace on the his catheter where a clear His signal is seen – preferably the distal to avoid direct atrial capture (see caveats below)
Ensure you have at least 3 ECG leads on screen to identify QRS morphology
Set the output to the maximum on the stimulator (usually 20 mA) and start pacing at a rate only slightly faster than the sinus rate to allow consistent capture. Going fast can lead to decremental issues (see caveats below)
Reduce output while observing QRS morphology (width).
When there is a change in QRS width, measure stimulus to A time in both a narrow beat and a wide beat and compare.
If they are similar (extra-nodal response), an AP is present and if the are significantly different (nodal response), the the presence of an AP is unlikely.
Retest to confirm reproducibility
Caveats
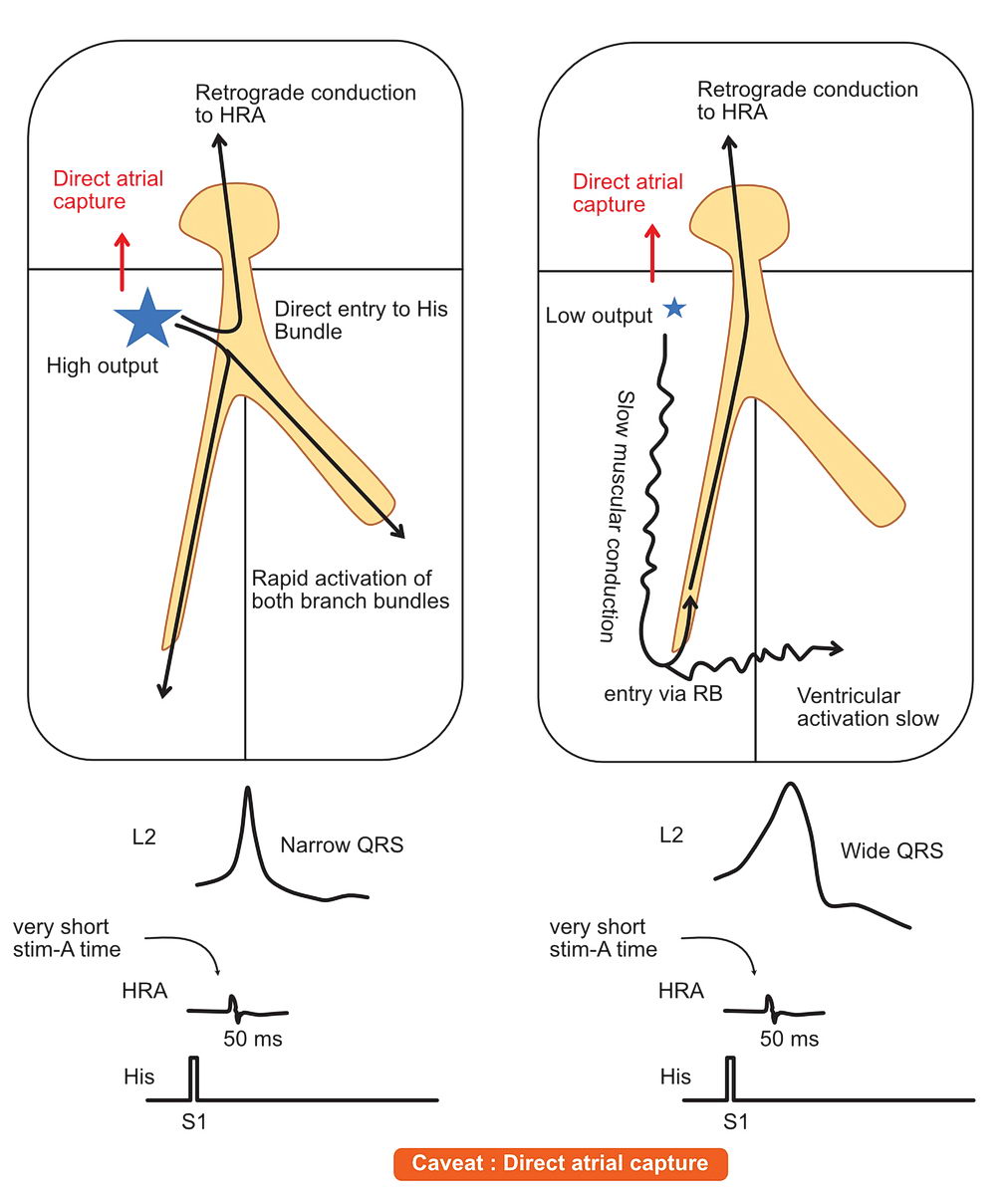
There are some caveats associated with this maneuver. The most common one is direct atrial capture by the catheter being too close to the the atrium. One can suspect direct atrial capture if the stimulus to A time is less than 80 ms during all phases of pacing. In this situation pacing should be done in a more distal pair of electrodes or the His catheter moved a little bit distal into the ventricle.
Common caveat of parahisian pacing : Direct atrial capture – which should be suspected when there is an abnormally short stim to A time
The other main caveat is the distance of the AP from site of pacing – so left lateral APs may falsely give a nodal response simply because the AP is far away. (but one should note the eccentric CS activation that would suggest a left lateral AP) The maneuver is most useful for septal APs
If the pacing electrodes are too ventricular, direct Right bundle capture may occur at both phases of the test – thus giving a false negative result
Tips
In addition to the initial diagnostic part, this maneuver is also useful to look for pathway conduction following ablation. A clear difference in pre and post ablation stimulus to A responses confirms successful abolition of retrograde AP conduction
If a doubt exists as to the result, another test that can be done is differential pacing– especially post ablation as you already have a flexible catheter in the heart. It is good practice to confirm loss of pathway conduction at the end of ablation using both techniques as they are complementary
Minutiae
Theoretically, during low out put pacing, because of the time that it takes for the signal to reach the His bundle, the His deflection should be visible after pacing. During high output, the His signal should be buried in the pacing impulse as the stimulus directly enters his bundle
In other-words, a visible (measurable) stimulus to His deflection time would indicate loss of direct his bundle capture and now if the stimulus to A time remains same, there is a pathway.
However, for practical purposes, this is very difficult to demonstrate as the His signal usually is buried in the pacing impulse unless a high fidelity filtering system is in place.
The other factor to consider is fusion (AV node + pathway conduction)- this should be suspected if the retrograde atrial activation sequence is changed during the two phases of the test. However again most changes are subtle and requires careful playing with calipers on multiple electrodes pairs which show atrial signals (CS, HRA, His etc…)