Putting premature ventricular complexes (PVCs) during narrow complex tachycardia is a very useful maneuver to narrow down the differential diagnosis of SVTs.
In a normal heart, the only connection between the atrium and ventricle (vice versa) is the AV node – his bundle complex.
During tachycardia, when the His bundle is refractory (I.e. immediately after seeing a His signal on the His catheter) any disturbance placed in the ventricle should not disturb the subsequent atrial signal – unlessthere is an additional connection between the atria and the ventricles.
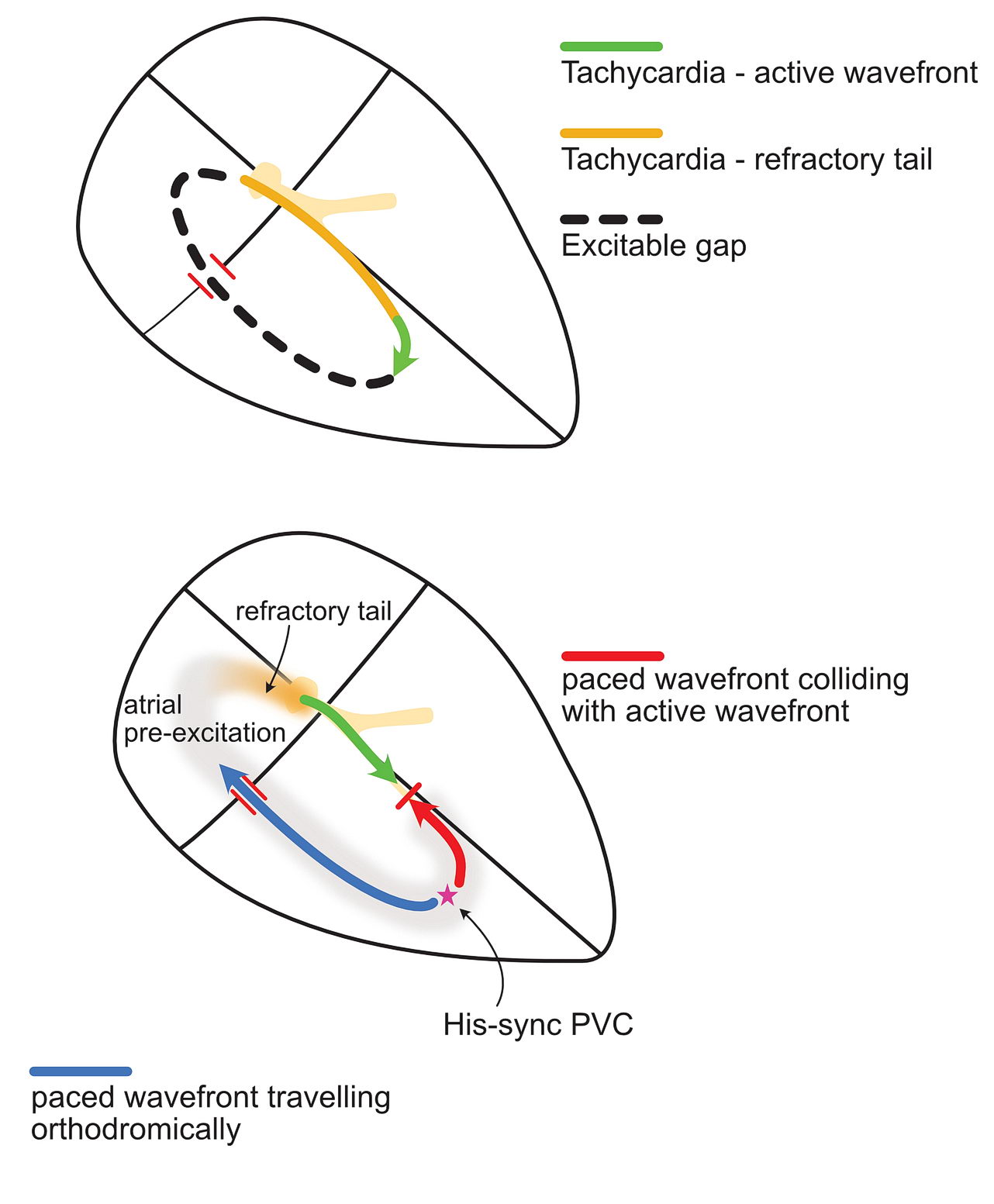
In other words, if there is an accessory pathway, putting a PVC during His refractoriness should change the timing of the next atrial signal as the PVC can ascend to the atrium via the accessory pathway. Look at the following diagram:
The top panel shows atrioventricular re-entry (AVRT) from an accessory pathway. The common form is orthodromic tachycardia - where the wavefront travels down the His bundle and comes back via the accessory pathway.
The bottom panel shows what happens when a PVC is introduced when the His bundle is refractory. The red wavefront collides with the incoming tachycardia green wavefront. The paced blue (orthodromic wave) travels up the accessory pathway to the atrium. Since this isearlier than the expected wave from the tachycardia, the atrial signal appears early - and is called atrial pre-excitation.
Why do we time it with the His signal? – because then we are sure that the His bundle is refractory i.e. unable to conduct.
Now lets look at an example tracing and study this further. Also recommended to read this section on entrainment as this is really got to do with entrainment. If you understood that – this is not a mystery.
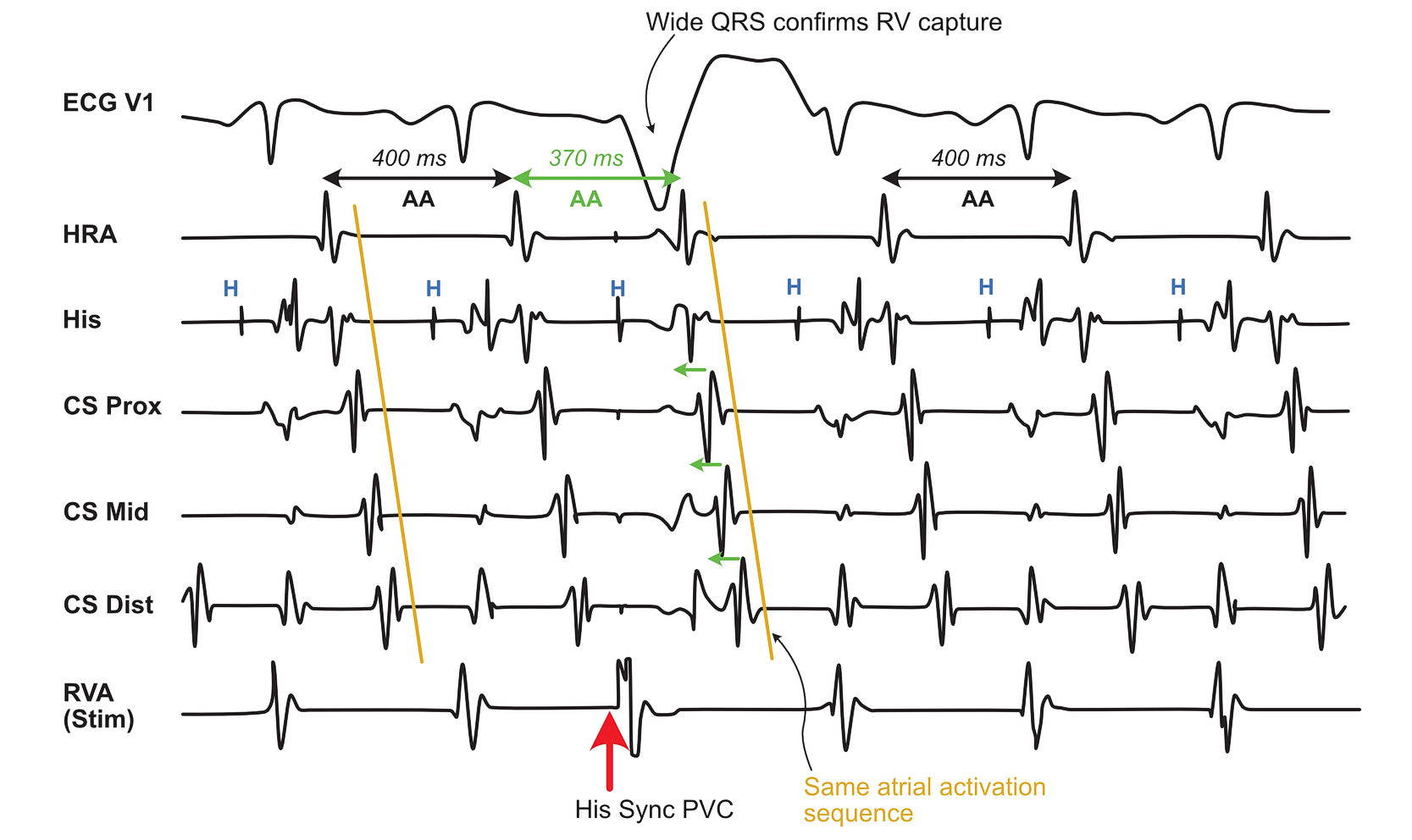
A short RP tachycardia is seen with concentric atrial activation. HRA is the earliest A - so a right sided concealed pathway is a possibility. A PVC is applied to the RV apex catheter in timing with the His deflection (Blue H). Ventricular capture is confirmed by the wide QRS complex of the paced beat. The subsequent atrial signal is advanced / pulled in (green arrows) by 30 ms. The pattern of atrial activation remains the same. Therefore one must conclude that there is an accessory pathway to the atrium. However this does not prove the tachycardia is due to the accessory pathway.
As shown in the diagram, the advancement of the atrial signal confirms the presenceof the pathway. To really prove that this pathway is participating in the tachycardia is by proving resetting as AVRT would be a re-entrant tachycardia.
Why do we need to prove it? Because if the pathway is a bystander, and the tachycardia is something else – we would be in trouble. Admittedly bystander pathways are rare – most of them do participate in the tachycardia – but knowing the principle of resetting and looking for it helps when faced with rarity !
Lets add some more measurements to the tracing :
Same tracing as above but now we have measured some additional intervals. The AH interval immediately following the paced beat is prolonged because the A was early and this led to decremental conduction in the AV Node. This leads to an increase in the AA interval immediately following the paced beat. This shows that whole tachycardia circuit is functionally connected - changing one interval affects the other - but the tachycardia continues i.e resets and continues . The VA interval usually remains same as most pathways do not have decremental properties. The additional observation is the prolonged post pacing interval. We are pacing from the right ventricular apex and the catheter may not be perfectly in the circuit and with the added decremental conduction in the AV Node, the post pacing interval is prolonged.
In real life, proving reset is difficult as the intervals are subtle. The advancement of the atrial signal with the same atrial activation sequence is good enough to say that the tachycardia is AVRT. However if the activation sequence has changed, then you may be dealing with a bystander or a pathway to pathway tachycardia
However, termination of tachycardia without an atrial signal proves that the tachycardia is indeed AVRT. Lets look at a schematic and a tracing.
Orthodromic AVRT. A PVC is applied when the His is refractory. The antidromic red wave collides with the green tachycardia wavefront. The orthodromic blue wave tries to get in to the atrium - but the pathway has still not recovered - so it is unable to do so and the tachycardia terminates. For this phenomenon to occur, there must be an accessory pathway AND it should be participating in the tachycardia.
Short RP narrow complex tachycardia - with eccentric atrial activation with a possibility of a left side concealed AP. His synchronous PVC terminating tachycardia without getting into the atrium. This confirms the presence of a pathway and its participation in the tachycardia.
Occasionally, one may observe the next A getting late – this is because the earlyPVC decrements in the accessory pathway. This type of APs are rare and can lead to incessant tachycardia as in persistent junctional re-entrant tachycardia – mostly seen in kids
This delayed A response is unique that it self proves the presence of the pathway AND its participation in tachycardia.
Since the pathway decrements, the VA interval (and therefore the RP interval on the ECG) is long and therefore PJRT comes in to the differential diagnosis of long RP tachycardia. This is discussed later.
Rarely, the post pacing interval may be very long – despite other evidence of accessory pathway conduction ( i.e. Pulled in A, same atrial activation sequence, Extra-nodal response in Parahisian pacing) – this could be due to the return beat coming down via a slow AV nodal pathway.
Practically how would you time the PVC?. Basically one selects a good surface ECG and times the delivery of the impulse by scanning back in decrements of 10 ms. The stimulator will calculate the position based on the sensed R wave and deliver the impulse. Generally a several tries need to be done and the EGMs carefully inspected for proper timing.
The impulse should be always delivered exactly when the His signal seen or before its inscription (within 20 ms) . This is ensures that the His is indeed depolarized and refractory.
The other thing to be sure is proper ventricular capture. This easily confirmed by a large QRS spike from the paced beat. However at times there is no RV apex catheter and ventricular pace is from the His distal – where the ventricular capture may be narrow and difficult to identify.
Timing of His Sync pacing. The impulse should be delivered just before the His is seen- this ensure that the His is depolarized and refractory. If it is delivered too early then the one risks the tachycardia wave would have gone too far from the pacing catheter. If the pacing is done after seeing the His signal, again runs the risk of tachycardia wave gone past the pacing catheter. The ideal window begins about 20 ms before the His spike.
So what about other forms of SVTs – ATs? AVNRTs? – in either of these, there is no obligatory connection between the atria and the ventricles to sustain tachycardia – hence His synchronous PVC has no effect – Unless there is a bystander pathway – which is not participating in the tachycardia – how would we suspect it – is by looking at both – the atrial advancement and activation sequence. (The atrium would advance but the activation sequnce would be different and there won’t be any resetting of tachycardia)
Effect of His sync PVCs on AVNRT and AT. In both types, the tachycardia has no active component with the ventricle. The ventricle merely gets activate by impulses coming down the His bundle. Therefore His synchronous PVCs just collide with the waveform and have no effect on the atria or tachycardia.
His synchronous PVCs for narrow complex tachycardia
Take home messages :
Termination of tachycardia – without A, confirms presence of AP AND its participation in tachycardia
Advancement of A (pulled in A) – confirms presence of AP but does NOT prove its participation.
Resetting and same activation sequence add evidence for pathway participation
Delayed A (pushed A) – confirms presence of decrementalAP AND proves its participation in tachycardia.