Delta wave pattern on the sinus ECGs of WPW give a clue as to the location of the accessory pathway. Knowing the pathway location will give an idea of the challenges associated with ablating such pathway and therefore enable the patient to make an informed choice. It also gives an idea on how the operator should approach the ablation. For example, mid-septal APs have a higher risk of AV block, Postero septal APs may be very difficult to ablate and the recurrence rates can be higher, left sided pathways may require arterial access or trans-septal access with added risk.
Therefore identification of the site of the AP is using the ECG is an essential skill. There several algorithms (most famous is the Arruda algorithm) to do this, but with a basic idea of actually where these APs are located, we can work out the ECG to locate the site of the pathway without remembering or using these algorithms. There are some simple additional rules to help with the diagnosis – which we will see after we have had a good look at the big picture of the ECG diagnosis.
Before looking at the ECG, we’ll look at where these accessory pathways live. The are small strands of myocardium linking the atria to the ventricles across the AV rings. These strands are usually epicardial but can be ablated from inside the heart at the atrial origin or at the ventricular insertion – depending on the technique used by the operator. These myocardial connections are common on the left side, and therefore most of the accessory pathways are left sided, crossing the mitral valve annulus. Right sided pathways (across the tricuspid valve ring) are relatively rare. Based on their location, accessory pathways are divided to left and right sided pathways first and then septal or free wall depending on their location on TV / MV ring.
Before we go further, a clarification of what anteior and posterior in regard to pathways need to be explained. On RAO view, the AV valves are slightly slanted forwards, therefore, the superior part of the valves lie anterior and inferior part of the valves lie posterior. Based on this, APs on the top part of the valve rings are called anterior pathways and on the bottom of the valve rings are called posterior pathways.
The RAO view shows the three main categorizations of accessory pathway location as defined by the altitude. Anterior is the superior aspect of the valve but called anterior because the valve rings are slightly tilted anterior. On the LAO view we see the location of the AP in relation to the septum and free wall. Mid septal APs are the only APs truly septal. Antero septal APs and Postero septal APs are slightly away from the true septum. Free wall APs are obvious and are not shown here. Note that left antero-septal APs are exceedingly rare because of the Aorto-Mitral continuity. Note : Antero-septal APs are close to the bundle of His. Mid septal APs are close to the AV node and slow pathway. Out of the two APs, risk of AV block during ablation is higher in Mid septal APs as they are close to the AV node. The thick fibrous insulation of the His bundle provides relative safety in this area - but comparative to non septal locations, still the risk of AV block is high.
This is classification of pathways as anterior and posterior is a bit confusing – therefore authors have suggested using superior and inferior – but the common usage still remains anterior and posterior.
The postero-septal APs are not actually true septal APs and therefore some authors have again suggested the term inferior para-septal APs – but again the old nomenclature persists. It has to be noted that in general, antero-septal APs means – right side antero-septal APs – as left antero-septal APs are exceedingly rare because of the presence of a the aortic valve and aorto-mitral continuity.
Position of accessory pathways in relation to the mitral and tricuspid valves. As noted in the text, posterior is also referred to as inferior and anterior as superior. RA = Right Anterior, RL = Right Lateral, RP = Right posterior, RPS = Right Postero-septal, MS=Mid septal, LA=Left Anterior, LL= Left lateral, LP=Left Posterior, LPS=Left Postero-septal. The yellow circle represents the His Bundle.
As we now know where the pathways are, lets work out the ECG. The first fundamental concept is that the ventricular activation in sinus rhythm is a fusion of pathway conduction and conduction through the normal system. The pathway conduction occurs rapidly – hence it pre-excites the ventricles. The ECG manifestation of pathway conduction is the delta wave.
The second fundamental concept is that because of the pathway insertion is directly to the myocardium, the ventricular activation begins at that point of AP insertion
The final result is the fusion of this focus with the impulse coming down the normal system. Therefore to really identify the position of the AP, we nee to look at morphology of the delta wave. In cases of subtle pre-excitation, this may be inaccurate as the delta wave contribution is very small.
The first step is to identify whether it’s a superior AP or an inferior AP. For that we need to look at the inferior limb leads of the ECG. A positive delta wave in all of these leads suggest that the the point of insertion is in the superior valve ring. (The pathway contribution is coming downwards).
Positive delta in inferior leads suggest that the AP is anterior (superior) as the (delta) wave is going downwards. The zone in light green denotes the potential areas of the AP in both left and right side. The relative degree of positivity in the leads give a clue to the side of the AP. If all three are equally positive then its closer to the mid line whereas more positivity of III will indicate a left anterior (superior) AP.
Negative delta ( and negative overall QRS complexes) in inferior leads suggest that the AP is posterior (inferior) as the wave is going upwards. The zone in light green denotes the potential areas of the AP in both left and right side. The relative degree of negativity in the leads give a clue to the side of the AP. If all three are equally negative then its closer to the mid line. A deeply negative lead II is suggestive of an AP crossing in the CS
The next step is to identify the left/right side of the AP by looking at the precordial leads – specifically V1 and V6.
The precordial leads in a left side accessory pathway. The pre-excitation wave travels towards the right side and therefore the V1 (along its delta wave) is very tall and prominent. V6 is considerably blunted and is not tall as expected without pre-excitation.
The pre-excitation waveform is traveling towards the left side and therefore the QRS complexes along with the delta wave is negative in V1 and positive in V6.
From the above it would be logical to state that left side APs show RBBB patternand right side APs show LBBB pattern
It is absolutely necessary to understand that this is of a similar patternto the bundle branch blocks – but have nothing to do with the bundles. Use of this type of nomenclature is discouraged
From the above description it is apparent that we can simply workout the ECG of WPW using the limb and precordial leads. But there are some things to remember facilitating diagnosis.
V1 – it is important to note the delta wave AND the R/S ratio. The delta polarity should match the R/S ratio. Hence all left side APs would be R>S with a positive delta wave. If they differ – it could be due to insufficient pre-excitation
A negative delta in V1 indicates a right side AP. The transition point to positivity indicates whether it is septal or free wall. Very early transition ( by V2) indicates a septal AP whereas a late transition indicates a right free wall AP
A negative delta in aVL & I indicate a left lateral AP – with corresponding changes in other leads.
A deeply negative limb lead II delta indicates that the AP is in the coronary sinus
Right postero-septal APs have negative delta V1 transiting to positive in V2 and Inferior lead III more negative than Lead II
Antero-septal APs have positive delta waves in inferior leads (the opposite of postero-septal APs) and a negative delta in V1 – which transitions to positive in V2. (Remember antero-septal APs are right side only)
Mid septal APs can be tricky depending on the exact location usually its a mixed picture in the inferior leads but again V1 negative, transiting to positive in V2. Lead I / aVL will give additional clues to whether they are left or right sided.
Lets now see some example ECGs
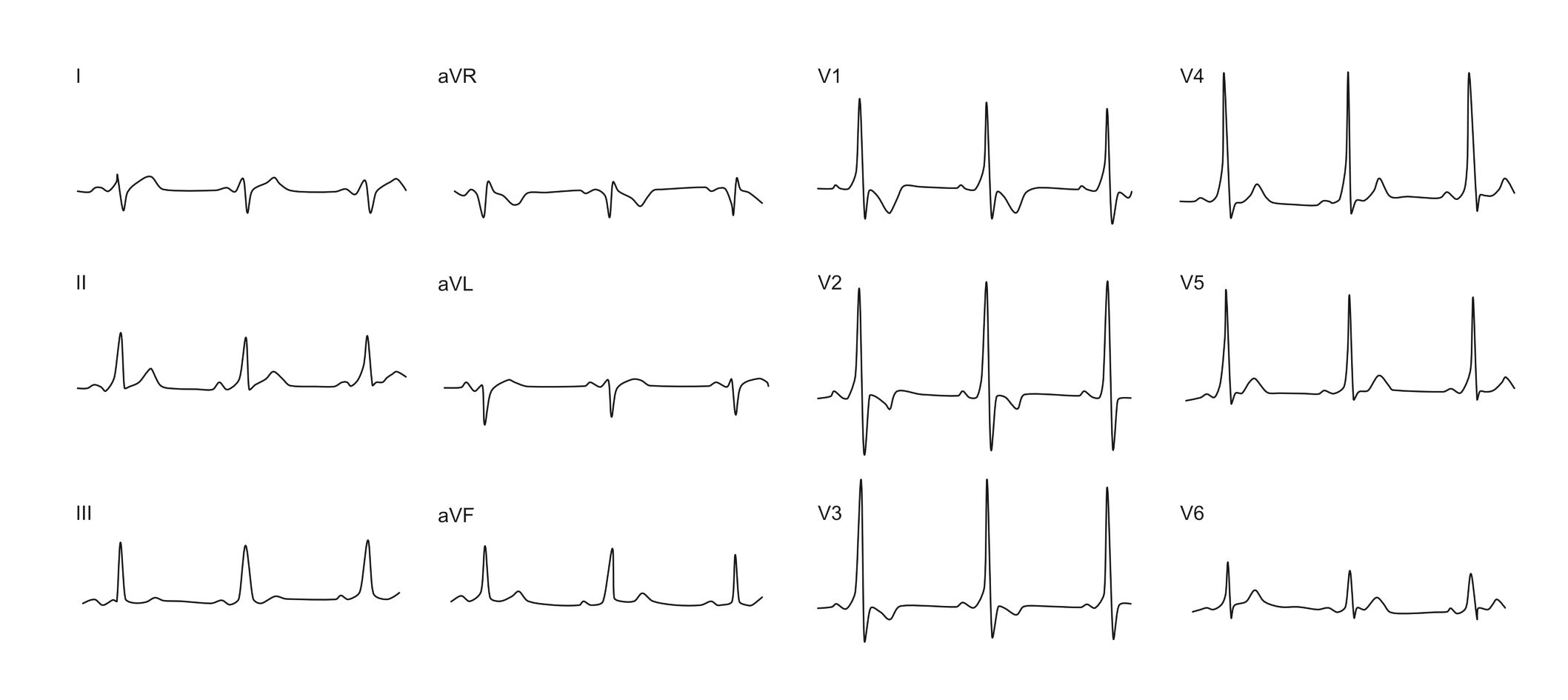
Left antero-lateral AP. Inferior leads are almost all equally positive - suggesting that the AP is superior (anterior). V1 delta (and R/S ratio) is positive suggesting that AP is on the left side. aVL is clearly negative suggesting that its going away from aVL - putting all this together, the AP is in the antero lateral part of the mitral ring - likely between 12 o-clock and 2 o-clock
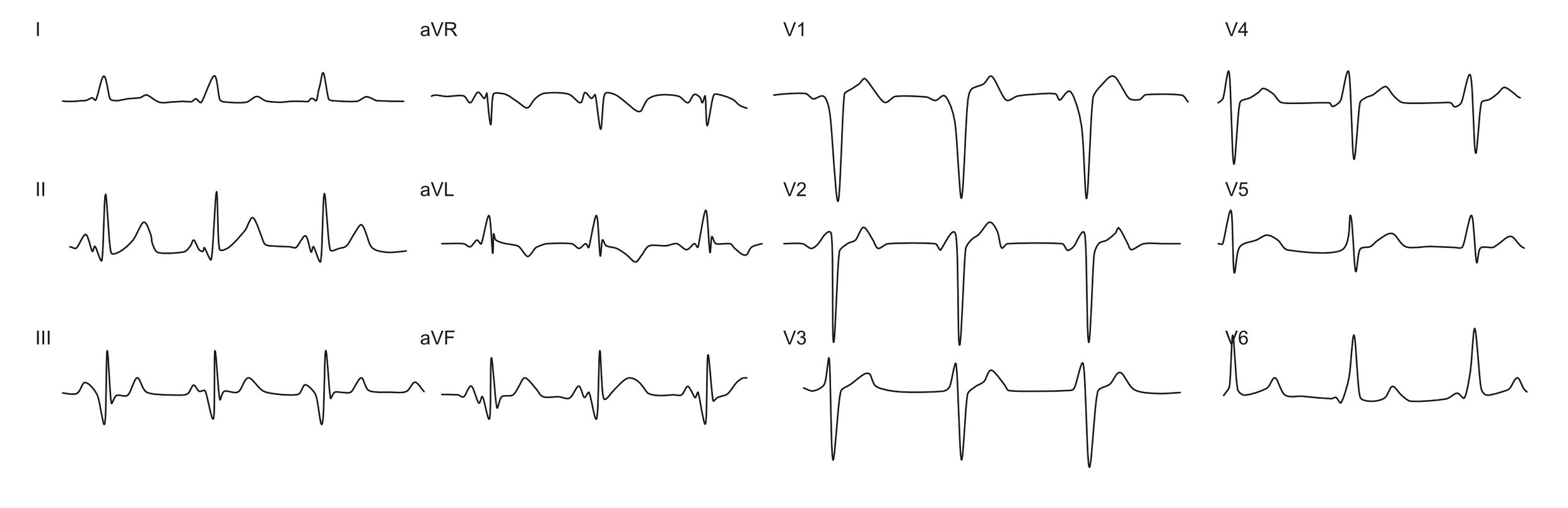
Right postero-septal AP. The inferior leads are in general negative - most negative being lead III least negative (biphasic) in lead II. This suggests that the AP is inferior (posterior) on the valve ring and predominantly going away from lead III. V1delta and the R/S ratio is negative - however it rapidly transitions to a positive delta and positive R/S ratio in V2 - this is characteristic of a right septal location and with the inferior lead findings, confirms that its a right postero-septal AP. (Note how aVL and lead I are positive suggesting that the depolarization from the AP is coming towards them - again with a right side or septal location)
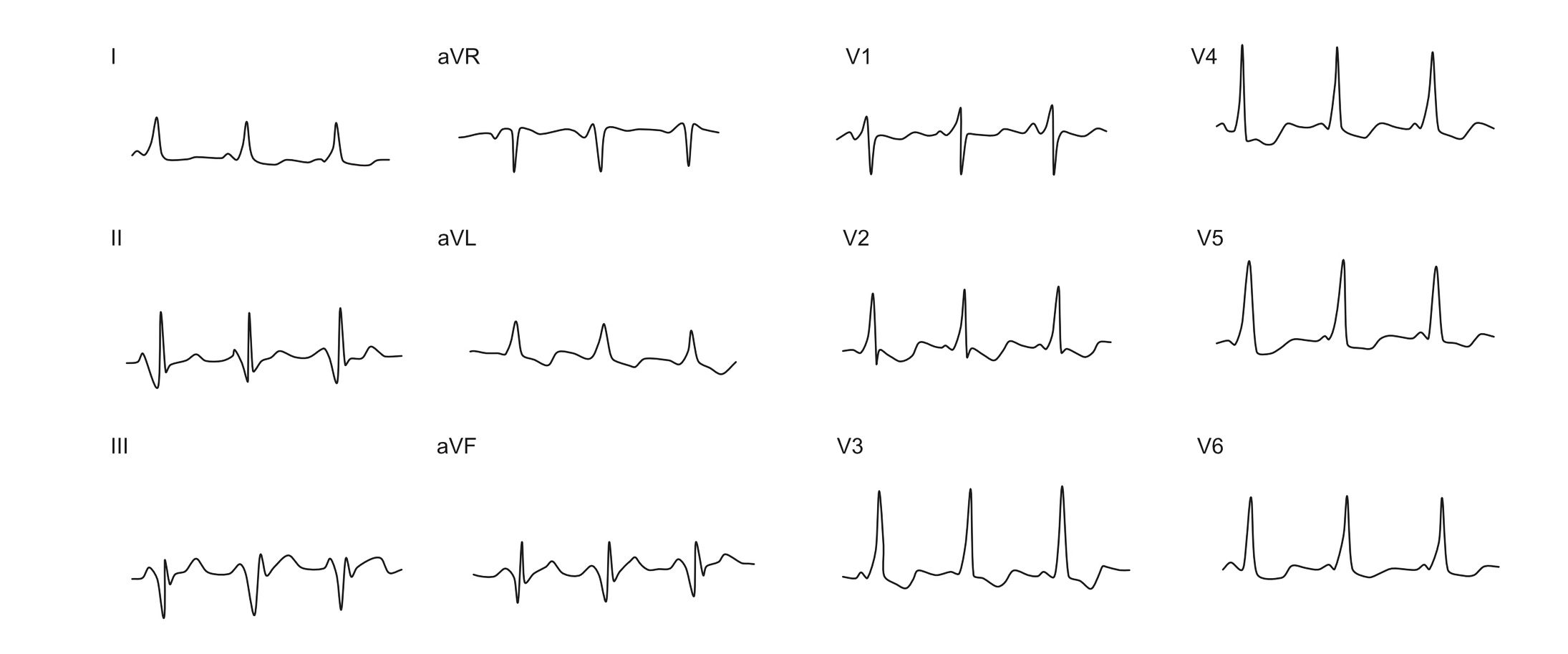
Right inferior AP. The inferior leads are almost equally negative - suggesting AP depolarization coming from inferior (posterior). In V1, the delta is clearly negative and R/S ratio remains negative until V5. This points towards a right side location of AP depolarization versus left. Given the combined findings of the above lead groups, the conclusion is a right inferior AP. An additional clue as to this has to be a right sided a AP is the slight excess negativity of lead II and strongly positive delta in aVL suggesting that a right sided inferior location for AP depolarization
Left postero-septal AP. Inferior leads are negative with more negativity in lead III. This suggests an inferior (posterior location). V1 shows a clear positive delta wave but the ratio is still negative.
The ratio becomes positive from V2 A right sided AP cannot explain this. Given the above, this is a left sided postero - septal AP. ( A positive delta in V1 suggests a left side location but the discrepancy in the R/S ratio is explained by the insufficiency of pre-excitation. )