In this section we will look at some common uses of entrainment in routine EP.
The first example we will be looking is entrainment of an orthodromic AVRT from the ventricle. This is a very common procedure – but very few realize hidden principles of entrainment it contains.
Given below is an orthodromic AVRT from a right sided AP, being entrained from the ventricle via a catheter in the RV apex.
Entrainment of orthodromic AVRT from the ventricle. The tachycardia cycle rate in the atrium has increased to the paced rate and the activation sequence remains same. Therefore we have some evidence for entraining the atrium from the ventricle. The post pacing interval - TCL is less than 120 ms, and by convention this shows our pacing site is quite close to the circuit. (In comparison to AVNRT). How about fusion - is there ECG fusion? - Unfortunately there is NO ECG fusion - the paced complex is completely the paced complex - as the antidromic paced wave collides within the conduction system with the incoming wave via the His bundle. Therefore there is no exiting tachycardia wavefront to fuse with the paced wave. (This is the case even for left side APs as the conduction system carries the paced impulse fast to the circuit). Hence this is an example of concealed entrainment. The last QRS resulting from the last pace (yellow circle) appears similar to the native tachy QRS and is this is a partial fulfillment of a major criterion for entrainment. (The bottom schematic shows how this happens)
Since we have no surface ECG fusion - we CANNOT demonstrate progressive fusion at ECG level.
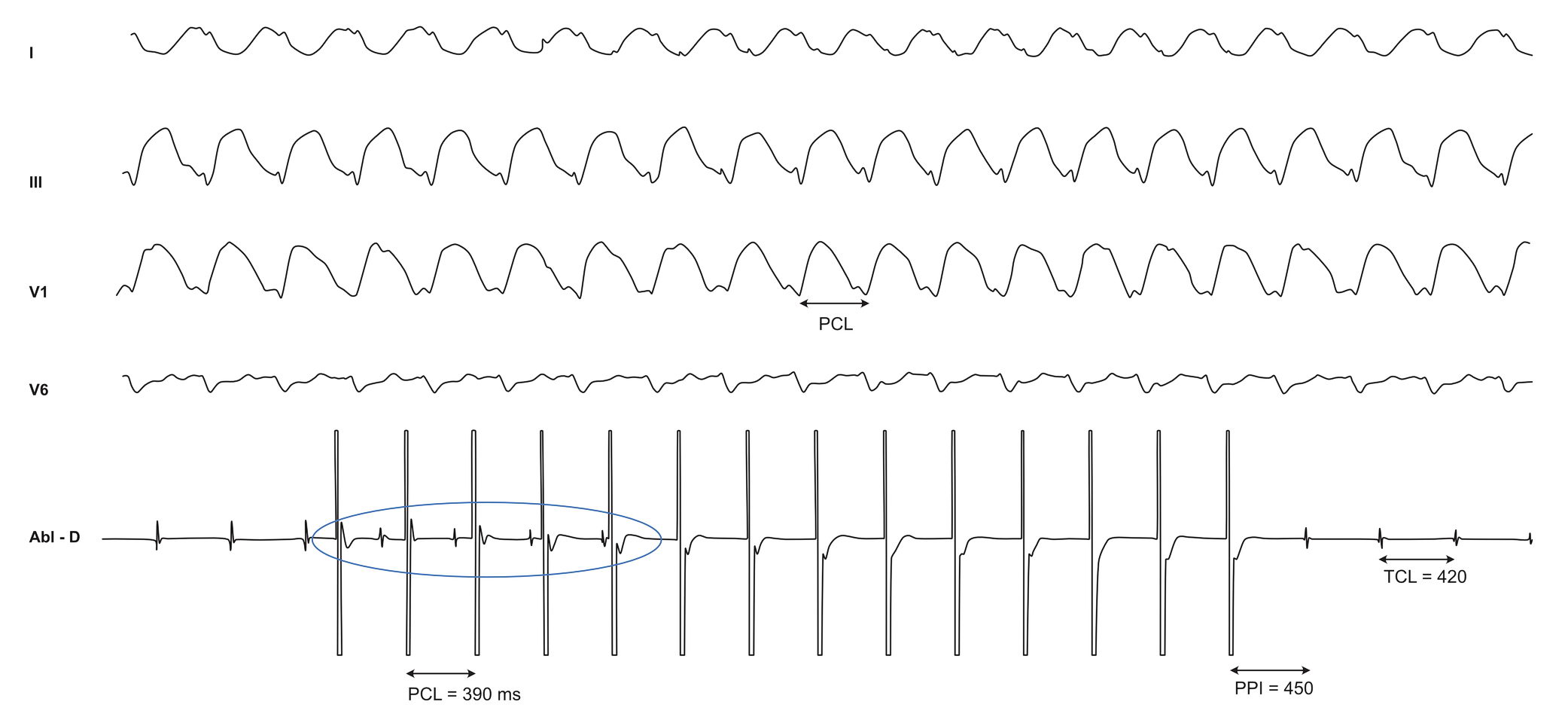
The next example we are going to consider is a VT. This patient had a haemodynamically stable VT -which was subjected to entrainment at different sites.
We can see a wide complex tachycardia (which was a VT) at a cycle length of 420 ms. The ablation catheter pacing at 380 ms at a site which we think is may near or in the VT circuit. The tachycardia is accelerated to the paced rate but the ECG morphology is different. The last entrained beat (circled in yellow) is similar to the native tachycardia beat and the post pacing interval is 472 ms. The ECG shows constant fusion (as it is a different morphology) and the last entrained beat is similar to the tachycardia so this fulfills a major criterion for entrainment. PPI-TCL is 50 ms, and given the presence of manifest fusion, we can conclude this pacing site is out of the inner channel of the circuit.
As explained, the pacing site is out of the circuit – but manifest fusion and native appearing last entrained beat confirms that the tachycardia is indeed a re-entrant one.
Same tachycardia, now being paced with the ablation catheter in a different place. Here we see the tachycardia accelerate to the paced speed but the ECG remains identical. Upon cessation of pacing, the tachycardia returns to native cycle length. The PPI-TCL is now 30 ms. Based on this the pacing catheter must be within or very close to the circuit. Absence of manifest ECG fusion indicates that this site is protected and the paced impulse has to exit via the natural exit of the tachycardia. Hence this is concealed entrainment in a site within a protected channel of the circuit. An additional observation is the time which it takes for the paced impulse to begin penetrating the excitable gap. (Blue circle) Although right within the circuit, because our pacing does not start within a excitable gap, it takes time for the pacing impulse to "meet" the excitable gap. The visible recording in the pacing channel indicates the native tachycardia is still going on an our paced impulse merely falls on the refractory tail without myocardial capture. This exemplifies the need to pace slightly fast to catch the excitable gap, even when you are in the circuit.
The above two of many possible outcomes of entraining a scar related VT. More of the possibilities are discussed in the section Scar VT – but the basic principles of entrainment are same for each outcome.